- Published on
Surgery - Colorectal Resection, Left Hemicolectomy
Indications
Elective: The most typical indications include tumors of the proximal sigmoid colon and descending colon. extreme diverticular illness.
Emergency: In rare cases, recommended for ischaemia, hemorrhage, perforation, or blockage.
Anatomy
The peritoneum covers the anterior surface and sides of the descending colon, which extends from the splenic flexure to the sigmoid colon at the pelvic brim. The phrenicocolic ligament, which runs parallel to the larger omentum and is closely linked to the spleen and tail of the pancreas, connects the splenic flexure to the diaphragm. Associated with the left kidney, lumbar region, and iliac fascia posteriorly.
vascular The sigmoid colon, the superior two thirds of the rectum, and the descending colon are all supplied by the inferior mesenteric artery (IMA). The IMA gives rise to the left colic artery, and the marginal artery (of Drummond) is partially formed by its ascending branch. The portal system receives venous drainage from the inferior mesenteric vein.
Investigations
Imaging: CT scan for staging and diagnosis; barium enema; erect CXR; abdominal radiograph.
Colonoscopy and sigmoidoscopy: For biopsy and diagnosis. Colonic lesion extraluminal localization can be facilitated by endoscopic tattooing.
Bloods: FBC, U&Es, clotting, and crossmatch prior to surgery. general evaluation of anesthesia. dosage of thromboprophylaxis, a preventive antibiotic. Preparing the bowels may be necessary.
After surgery: Better recuperation, prompt resumption of food and drink, mobilization, and effective analgesia. IV fluids are continued until oral intake is sufficient. Maintaining a precise record of fluid equilibrium is necessary. prevention of DVT. Revert to an NG tube and IV fluids until symptoms of post-operative ileus subside. In the postoperative phase, if there are any indications of a systemic disturbance, an anastomotic leak must be ruled out.
Procedure
Position: Lloyd Davis/modified lithotomy.
Access: Laparoscopic or midline incision methods. The contents of the abdomen are examined, looking for signs of liver metastases or swollen lymph nodes, and the small bowel is packed away from the left hemicolon.
The division of the peritoneal attachments at the white line of Toldt to the level of the splenic flexure mobilizes the descending colon. The spleen, left ureter, gonadal arteries, kidney, pancreas, and fourth portion of the duodenum must all be carefully avoided. Enough transverse colon mobilization occurs to allow for a tension-free anastomosis.
Ligation of vessels: The inferior mesentery artery and left colonic branches are located by dissecting the mesentery. The artery supply to the proximal and distal edges is then preserved by isolating, ligating, and dividing them.
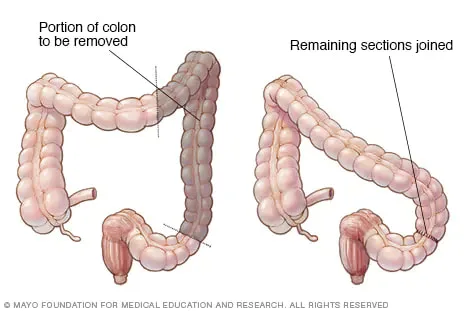
Resection of bowel segment: The colonic segment and its accompanying mesentery are removed, and the bowel is clamped and separated, usually using linear staples.
Restoring intestinal continuity involves performing a handsewn or stapled anastomosis between the descending colon and the rectosigmoid colon. Closing the mesenteric defect prevents internal herniation.It is possible to create an aproximal defuncting stoma to shield the distal anastomosis.
Conclusion: Hemostasis is verified. Usually, a drain is installed. Sutures or clips are used to finish the skin closure once the abdominal wall is mass closed.
Complications
bleeding, infection, ileus, anastomotic leak, hernias, and thromboembolism are examples of visceral injuries.
Indications
Elective: The most typical indications include tumors of the proximal sigmoid colon and descending colon. extreme diverticular illness.
Emergency: In rare cases, recommended for ischaemia, hemorrhage, perforation, or blockage.
Anatomy
The peritoneum covers the anterior surface and sides of the descending colon, which extends from the splenic flexure to the sigmoid colon at the pelvic brim. The phrenicocolic ligament, which runs parallel to the larger omentum and is closely linked to the spleen and tail of the pancreas, connects the splenic flexure to the diaphragm. Associated with the left kidney, lumbar region, and iliac fascia posteriorly.
vascular The sigmoid colon, the superior two thirds of the rectum, and the descending colon are all supplied by the inferior mesenteric artery (IMA). The IMA gives rise to the left colic artery, and the marginal artery (of Drummond) is partially formed by its ascending branch. The portal system receives venous drainage from the inferior mesenteric vein.
Investigations
Imaging: CT scan for staging and diagnosis; barium enema; erect CXR; abdominal radiograph.
Colonoscopy and sigmoidoscopy: For biopsy and diagnosis. Colonic lesion extraluminal localization can be facilitated by endoscopic tattooing.
Bloods: FBC, U&Es, clotting, and crossmatch prior to surgery. general evaluation of anesthesia. dosage of thromboprophylaxis, a preventive antibiotic. Preparing the bowels may be necessary.
After surgery: Better recuperation, prompt resumption of food and drink, mobilization, and effective analgesia. IV fluids are continued until oral intake is sufficient. Maintaining a precise record of fluid equilibrium is necessary. prevention of DVT. Revert to an NG tube and IV fluids until symptoms of post-operative ileus subside. In the postoperative phase, if there are any indications of a systemic disturbance, an anastomotic leak must be ruled out.
Procedure
Position: Lloyd Davis/modified lithotomy.
Access: Laparoscopic or midline incision methods. The contents of the abdomen are examined, looking for signs of liver metastases or swollen lymph nodes, and the small bowel is packed away from the left hemicolon.
The division of the peritoneal attachments at the white line of Toldt to the level of the splenic flexure mobilizes the descending colon. The spleen, left ureter, gonadal arteries, kidney, pancreas, and fourth portion of the duodenum must all be carefully avoided. Enough transverse colon mobilization occurs to allow for a tension-free anastomosis.
Ligation of vessels: The inferior mesentery artery and left colonic branches are located by dissecting the mesentery. The artery supply to the proximal and distal edges is then preserved by isolating, ligating, and dividing them.
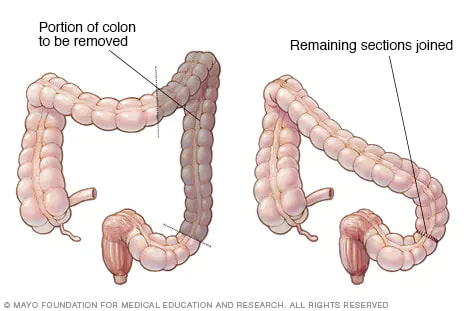
Resection of bowel segment: The colonic segment and its accompanying mesentery are removed, and the bowel is clamped and separated, usually using linear staples.
Restoring intestinal continuity involves performing a handsewn or stapled anastomosis between the descending colon and the rectosigmoid colon. Closing the mesenteric defect prevents internal herniation.It is possible to create an aproximal defuncting stoma to shield the distal anastomosis.
Conclusion: Hemostasis is verified. Usually, a drain is installed. Sutures or clips are used to finish the skin closure once the abdominal wall is mass closed.
Complications
bleeding, infection, ileus, anastomotic leak, hernias, and thromboembolism are examples of visceral injuries.
0 Comments
