- Published on
Surgery - Colorectal Resection, Low Anterior
Indications
Elective: Sigmoid or Rectal tumours, if adequate margins above the anal sphincter complex.
Anatomy
Starting at the level of the third sacral vertebra, the rectum (12 cm) descends and lies in the sacrococcygeal curve until it reaches the tip of the coccyx. After that, it abruptly turns back into the anal canal. The autonomic plexus, hypogastric nerves, and presacral (Waldeyer) fascia divide the rectum from the mesorectum. There are lymphatics and fatty tissue in it, and complete mesorectal excision has been demonstrated to lower the risk of local recurrence.
Vascular: The superior rectal artery receives blood from the inferior mesenteric artery to supply the upper rectum. The internal iliac artery is the source of the middle and inferior rectal arteries, which supply the lower rectum. The superior, middle, and inferior rectal vessels—the sites of portacaval anastomosis—are the drains of the rectal venous plexus.
Lymphatics: Drainage reaches the para-aortic nodes via following the inferior mesenteric artery.
Investigational studies
Imaging: CT, MRI, endorectal ultrasound: For planning/assessing appropriateness for anterior resection, as well as staging.
Pre-op: Chemoradiotherapy prior to surgery may be necessary (reduces local recurrence).
Bowel preparation, bloods: FBC, U&Es, clotting and crossmatch, general anaesthetic assessment and relevant investigations.
Close observation follows surgery. prevention of DVT.
Actions
The patient is arranged in an elongated Lloyd-Davis posture.
Incision: Laparoscopic procedures or lower or longer midline incisions are both possible.
Examining the abdominal cavity and determining the size and location of the tumor constitute the process of mobilizing the colon. The ureter and gonadal veins are carefully identified as the left colon and sigmoid mesentery are mobilized. Mobilization of the splenic flexure can be necessary.
The inferior mesenteric artery and vein are split, dissected, and ligated in order to mobilize the rectum.Using a stapler, the sigmoid, mesocolon, and sigmoid are separated, generally at the apex. The plane between the mesorectum and the sacral fascia can then be seen by pulling the rectum forward. The rectum is further dissected laterally and posteriorly, giving rise to a distinctive bilobed look.The plane between the anterior mesorectum and the seminal vesicles in the male and vagina in the female is then developed by the division of the peritoneum right above the apex of the rectovesical or rectouterine pouch.
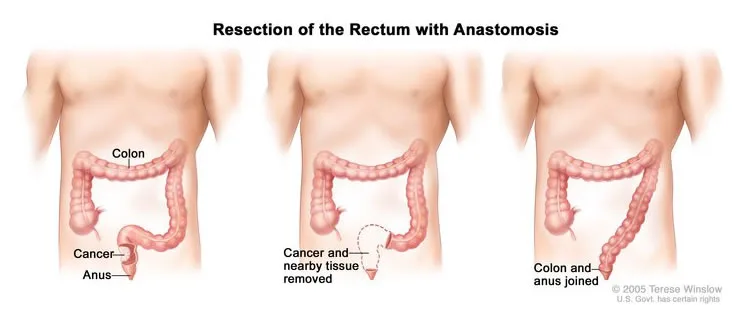
Resection: A minimum of 2 cm of adequate clearance is required both proximally and distally from the tumor.
At the proximal and distal resection sites, clamps are positioned. Using a proctoscope, the lower rectum and anus are cleaned with an antiseptic solution. The bowel is then split between the proximal and distal clamps using a stapler.
Anastomosis: A circular staple gun is typically used by surgeons. An helper inserts the gun PR and advances the rod through the staple line's center. The anvil, which is the receiving end of the stapler gun, is wrapped with sutures around the proximal bowel end. The stapler is closed and fired to ensure that there is no twisting, resulting in the excision of a ring of intestine and the stapleing of the two ends together. The tissue "donuts" that are removed are sent to histology in addition to being inspected to make sure the rings are complete. By using air sufflation PR to conduct a leak test, the anastomosis can be verified.
Closure: Typically, a pelvic drain is left in place. There are non-absorbable stitches used to seal the abdominal wall. Sutures or clips finish the skin closing process. It is common practice to create a malfunctioning ileostomy to redirect stool contents during anastomotic recovery.
Complications
bleeding, ileus, anastomotic leak, infection, and abscess. The frequency and severity of bowel movements
Indications
Elective: Sigmoid or Rectal tumours, if adequate margins above the anal sphincter complex.
Anatomy
Starting at the level of the third sacral vertebra, the rectum (12 cm) descends and lies in the sacrococcygeal curve until it reaches the tip of the coccyx. After that, it abruptly turns back into the anal canal. The autonomic plexus, hypogastric nerves, and presacral (Waldeyer) fascia divide the rectum from the mesorectum. There are lymphatics and fatty tissue in it, and complete mesorectal excision has been demonstrated to lower the risk of local recurrence.
Vascular: The superior rectal artery receives blood from the inferior mesenteric artery to supply the upper rectum. The internal iliac artery is the source of the middle and inferior rectal arteries, which supply the lower rectum. The superior, middle, and inferior rectal vessels—the sites of portacaval anastomosis—are the drains of the rectal venous plexus.
Lymphatics: Drainage reaches the para-aortic nodes via following the inferior mesenteric artery.
Investigational studies
Imaging: CT, MRI, endorectal ultrasound: For planning/assessing appropriateness for anterior resection, as well as staging.
Pre-op: Chemoradiotherapy prior to surgery may be necessary (reduces local recurrence).
Bowel preparation, bloods: FBC, U&Es, clotting and crossmatch, general anaesthetic assessment and relevant investigations.
Close observation follows surgery. prevention of DVT.
Actions
The patient is arranged in an elongated Lloyd-Davis posture.
Incision: Laparoscopic procedures or lower or longer midline incisions are both possible.
Examining the abdominal cavity and determining the size and location of the tumor constitute the process of mobilizing the colon. The ureter and gonadal veins are carefully identified as the left colon and sigmoid mesentery are mobilized. Mobilization of the splenic flexure can be necessary.
The inferior mesenteric artery and vein are split, dissected, and ligated in order to mobilize the rectum.Using a stapler, the sigmoid, mesocolon, and sigmoid are separated, generally at the apex. The plane between the mesorectum and the sacral fascia can then be seen by pulling the rectum forward. The rectum is further dissected laterally and posteriorly, giving rise to a distinctive bilobed look.The plane between the anterior mesorectum and the seminal vesicles in the male and vagina in the female is then developed by the division of the peritoneum right above the apex of the rectovesical or rectouterine pouch.
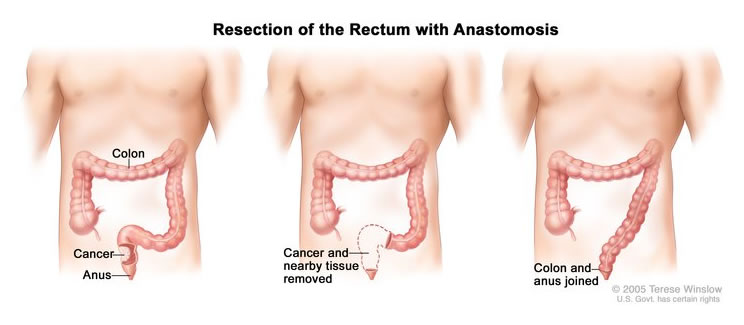
Resection: A minimum of 2 cm of adequate clearance is required both proximally and distally from the tumor.
At the proximal and distal resection sites, clamps are positioned. Using a proctoscope, the lower rectum and anus are cleaned with an antiseptic solution. The bowel is then split between the proximal and distal clamps using a stapler.
Anastomosis: A circular staple gun is typically used by surgeons. An helper inserts the gun PR and advances the rod through the staple line's center. The anvil, which is the receiving end of the stapler gun, is wrapped with sutures around the proximal bowel end. The stapler is closed and fired to ensure that there is no twisting, resulting in the excision of a ring of intestine and the stapleing of the two ends together. The tissue "donuts" that are removed are sent to histology in addition to being inspected to make sure the rings are complete. By using air sufflation PR to conduct a leak test, the anastomosis can be verified.
Closure: Typically, a pelvic drain is left in place. There are non-absorbable stitches used to seal the abdominal wall. Sutures or clips finish the skin closing process. It is common practice to create a malfunctioning ileostomy to redirect stool contents during anastomotic recovery.
Complications
bleeding, ileus, anastomotic leak, infection, and abscess. The frequency and severity of bowel movements
0 Comments
