- Published on
Surgery - Colorectal Resection, Right Hemicolectomy
Indications
Elective: Most frequently, appendiceal neoplasms, such as carcinoids >2 cm, or colonic neoplasms (caecum, ascending colon, or hepatic flexure). When hepatic flexure or transverse colon tumors are involved, extended right hemicolectomies are done. Crohn's disease is another.
Emergency: Recommended in cases of caecal volvulus or diverticulitis, as well as right colonic obstructive lesions, perforations, hemorrhages, or ischemia. In cases of severe appendicitis where the caecum is affected, ileocaecal resection or limited right hemicolectomy may be required.
Anatomy
From the caecum to the hepatic flexure, the ascending colon ascends (15 cm long). After that, it suddenly bends forward and to the left to form the transverse colon. Its anterior surface and sides are covered by the peritoneum, making it retroperitoneal. The right kidney, duodenum, and gonadal arteries, as well as the right ureter, are crucial structures to recognize and protect during surgery.
vascular The right colic, middle colic, and ileocolic arteries are the branches of the superior mesenteric artery that supply the arterial supply. Variable venous drainage enters the portal circulation mostly by the ileocolic, right colic, and middle colic veins.
Investigations
Imaging: CT scan, erect CXR, and abdominal radiograph: diagnosis and staging.
Colonoscopy: Polyp, tumor, inflammatory bowel, etc. diagnosis and biopsies.
Bloods: FBC, U&Es, clotting, crossmatch, preoperative.
evaluation of general anesthesia and thromboprophylaxis.
Post-op: Following elective surgery, improved recovery involves an early return to food and drink, prompt mobilization, effective analgesia, and close monitoring of the FBC, electrolytes, and urine output. Should there be indications of postoperative ileus, return to the traditional oral NG tube feeding regimen and gradually introduce liquids and solids as tolerated. Keep up the thromboprophylaxis.
Procedure
Lie down or do a modified lithotomy.
Access: Laparoscopic technique, transverse incision, or midline incision. The small intestine is packed up and the intra-abdominal contents evaluated.
Mobilize: Approaches from medial to lateral or lateral to medial are applied.
Lateral to medial: The division of the hepatocolic ligament mobilizes the hepatic flexure and inclines the right colon's lateral peritoneal attachments (white line of Toldt). identifying and avoiding the ureter, gonadal, and duodenum with caution. cautious removal of the right plane in front of Gerota's fascia. larger omentum dissection from the transverse colonic region that needs to be split.
Ligation of vessels: The ileocolic and right colic vessels are ligated and separated after the mesentery from the terminal ileum to the transverse colon is thoroughly dissected. It might also be necessary to divide the middle colic artery's right branches.
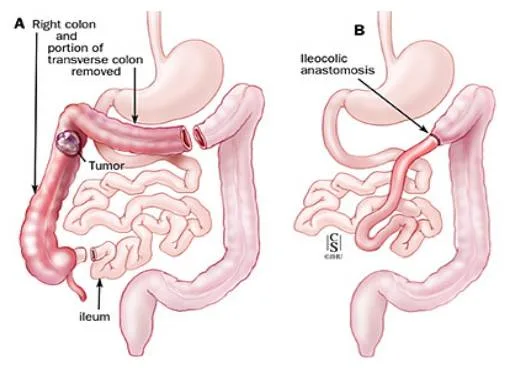
Resection of bowel segment: Clamps are positioned at both ends of the length that needs to be resected after measuring the amount of adequate clearance from the lesion. Linear staplers are frequently used to separate the gut, and the right colon is submitted for histology.
Restoring intestinal continuity: Healthy, well-vascularized, and tension-free bowel ends are required for bowel anastomosis. Using sutures or staples, the terminal ileum is anastomosed to the transverse colon in one or two layers, either side-to-side, end-to-end, or end-to-side. To stop internal herniation, the mesenteric defect is sealed.
Closure: A drain could remain in place. Mass closure after haemostasis confirmation.
Sutures or clips finish the skin closing process.
Complications include incisional hernias, thrombosis, ileus, abscess, wound infection, and anastomotic leak.
Indications
Elective: Most frequently, appendiceal neoplasms, such as carcinoids >2 cm, or colonic neoplasms (caecum, ascending colon, or hepatic flexure). When hepatic flexure or transverse colon tumors are involved, extended right hemicolectomies are done. Crohn's disease is another.
Emergency: Recommended in cases of caecal volvulus or diverticulitis, as well as right colonic obstructive lesions, perforations, hemorrhages, or ischemia. In cases of severe appendicitis where the caecum is affected, ileocaecal resection or limited right hemicolectomy may be required.
Anatomy
From the caecum to the hepatic flexure, the ascending colon ascends (15 cm long). After that, it suddenly bends forward and to the left to form the transverse colon. Its anterior surface and sides are covered by the peritoneum, making it retroperitoneal. The right kidney, duodenum, and gonadal arteries, as well as the right ureter, are crucial structures to recognize and protect during surgery.
vascular The right colic, middle colic, and ileocolic arteries are the branches of the superior mesenteric artery that supply the arterial supply. Variable venous drainage enters the portal circulation mostly by the ileocolic, right colic, and middle colic veins.
Investigations
Imaging: CT scan, erect CXR, and abdominal radiograph: diagnosis and staging.
Colonoscopy: Polyp, tumor, inflammatory bowel, etc. diagnosis and biopsies.
Bloods: FBC, U&Es, clotting, crossmatch, preoperative.
evaluation of general anesthesia and thromboprophylaxis.
Post-op: Following elective surgery, improved recovery involves an early return to food and drink, prompt mobilization, effective analgesia, and close monitoring of the FBC, electrolytes, and urine output. Should there be indications of postoperative ileus, return to the traditional oral NG tube feeding regimen and gradually introduce liquids and solids as tolerated. Keep up the thromboprophylaxis.
Procedure
Lie down or do a modified lithotomy.
Access: Laparoscopic technique, transverse incision, or midline incision. The small intestine is packed up and the intra-abdominal contents evaluated.
Mobilize: Approaches from medial to lateral or lateral to medial are applied.
Lateral to medial: The division of the hepatocolic ligament mobilizes the hepatic flexure and inclines the right colon's lateral peritoneal attachments (white line of Toldt). identifying and avoiding the ureter, gonadal, and duodenum with caution. cautious removal of the right plane in front of Gerota's fascia. larger omentum dissection from the transverse colonic region that needs to be split.
Ligation of vessels: The ileocolic and right colic vessels are ligated and separated after the mesentery from the terminal ileum to the transverse colon is thoroughly dissected. It might also be necessary to divide the middle colic artery's right branches.
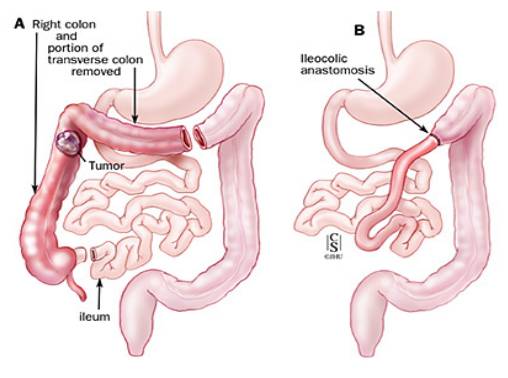
Resection of bowel segment: Clamps are positioned at both ends of the length that needs to be resected after measuring the amount of adequate clearance from the lesion. Linear staplers are frequently used to separate the gut, and the right colon is submitted for histology.
Restoring intestinal continuity: Healthy, well-vascularized, and tension-free bowel ends are required for bowel anastomosis. Using sutures or staples, the terminal ileum is anastomosed to the transverse colon in one or two layers, either side-to-side, end-to-end, or end-to-side. To stop internal herniation, the mesenteric defect is sealed.
Closure: A drain could remain in place. Mass closure after haemostasis confirmation.
Sutures or clips finish the skin closing process.
Complications include incisional hernias, thrombosis, ileus, abscess, wound infection, and anastomotic leak.
0 Comments
