- Published on
Surgery - Colorectal Resections, Abdomio Perineal Resection
Indications
lower rectum tumors that remain after chemotherapy and radiation therapy because they are too near the anal sphincter to get sufficient margins.
Anatomy
Starting at the level of the third sacral vertebra, the rectum (12 cm) extends anteriorly to the tip of the coccyx before descending and lying in the sacrococcygeal curve. Then, it makes a dramatic backward turn into the anal canal. The mesorectum is separated from the sacrum and hypogastric nerves posteriorly by the endopelvic (Waldeyer's) fascia, which is anteriorly located in the fascia of Denonvilliers, bladder, prostate, or vagina.
Vascular: The superior rectal artery receives blood from the inferior mesenteric artery to supply the upper rectum. The internal iliac artery is the source of the middle and inferior rectal arteries, which supply the lower rectum. The superior, middle, and inferior rectal vessels receive drainage from the rectal venous plexus. The portacaval connection is located in the rectal venous plexus.
Lymphatics: The anus below the dentate line drains to inguinal nodes, the lower can flow to internal iliac nodes, and the lymph from the upper and middle rectum drains to inferior mesenteric nodes.
Investigations
Imaging: CT, MRI, endorectal ultrasound: Used to plan and determine whether an abdominoperineal excision is appropriate.
Colonoscopy: To diagnose tissue and rule out concurrent tumors.
Blood tests, electrocardiograms, thromboprophylaxis, stoma marking, general anesthesia evaluation, and bowel preparation are all done prior to surgery.
Enhanced recovery following elective surgery includes an early return to eating and drinking, mobilization, effective analgesia, IV fluids until oral intake is sufficient, and monitoring of the whole blood count, electrolyte levels, and urine output. Maintain wound and stoma care, thromboprophylaxis, and education.
Procedure
The patient is positioned in the Lloyd Davies manner. The anal orifice is closed with sutures.
Lower midline incision, or laparoscopic procedures are also an option.
Mobilization: Similar to a low anterior resection, the left colon and sigmoid are mobilized. There is a division in the inferior mesenteric vein and artery. The rectum is dissected and mobilized, and the entire mesorectal region is removed down to the levator ani muscles. During the perineal phase, the anoccygeal ligament is divided posteriorly by making an oval incision around the anus. After this, the incision is made deeper into the muscle till it connects to the surgical site on the abdomen.
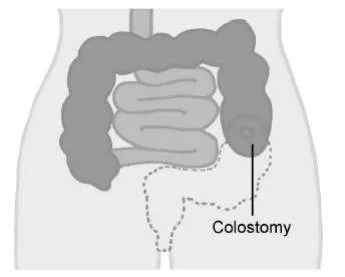
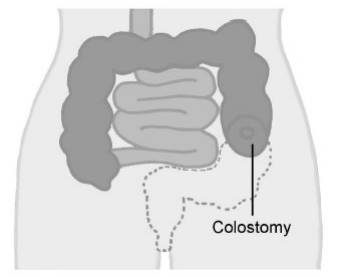
The anus and rectum are removed from the perineal side after colon division. It is customary to create an end colostomy in the left iliac fossa.
Closure: An in situ pelvic drain may be used. Subcuticular sutures are used to close the perineal surface and there is a mass closure of the abdominal wall using clips or sutures to skin.
Complications
Bleeding, infection, stoma necrosis or perineal wound necrosis, ileus, bladder dysfunction or impotence as a result of nerve injury, hernia, DVT/PE, and recurrence.
0 Comments
