- Published on
Surgery - Coronary Artery Bypass Graft
Indications
Triple coronary vessel disease, left main stem coronary artery disease, and two coronary vessel disease with a proximal left anterior descending artery lesion are the three primary anatomical reasons for CABG.
In these patients, CABG reduces angina and increases long-term survival.
Anatomy
After emerging from the ascending aorta, the right coronary artery passes anteriorly between the right auricle and the pulmonary trunk before descending via the atrioventricular groove.
It passes posteriorly and anastomoses with the left coronary artery at the inferior heart boundary.
The ascending aorta gives rise to the left coronary artery, which splits into the left anterior descending and left circumflex arteries in the atrioventricular groove after passing posteriorly between the pulmonary trunk and the left auricle. The internal mammary artery originates from the subclavian artery and descends behind the costal cartilages along the pleura. It finishes at the sixth intercostal gap, when it splits into the musculophrenic and superior epigastric arteries.
Investigational studies
Prior to surgery: ECG, echocardiography, coronary angiography, and thallium perfusion scintigraphy. Bloods: crossmatch, clotting, U&Es, and FBC. general evaluation of anesthesia.
Close observation in an ITU setting following surgery. meticulous follow-up.
Actions
A median sternotomy was made. The heart, coronary vessels, and large vessels are exposed and examined during pericardial dissection. Nowadays, less invasive thoracotomy incisions are made in an effort to lessen the morbidity associated with sternotomy.
"On Pump" CABG: Cardiopulmonary bypass machines are utilized during cardiac surgery to oxygenate and circulate blood. Perfusionists operate these machines. Blood is taken out of the right atrium and redirected into the ascending aorta via a venous cannula, causing systemic hypothermia and the administration of IV heparin. The heart is given a cardioplegic solution to cause a hypothermic cardioplegic arrest so that surgery can be done.
"Off pump" CABG: The heart is allowed to continue beating by applying tissue stabilisers, which are devices, to the surgical site.
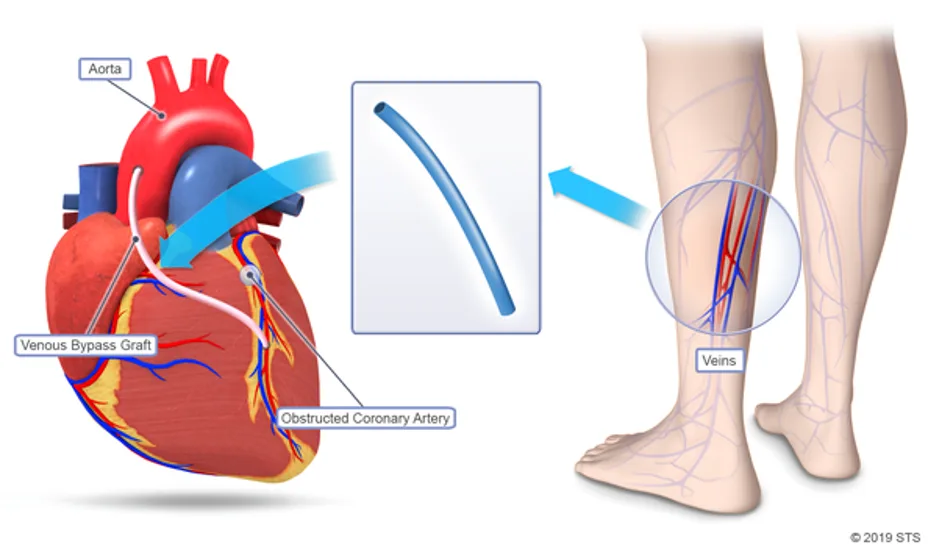
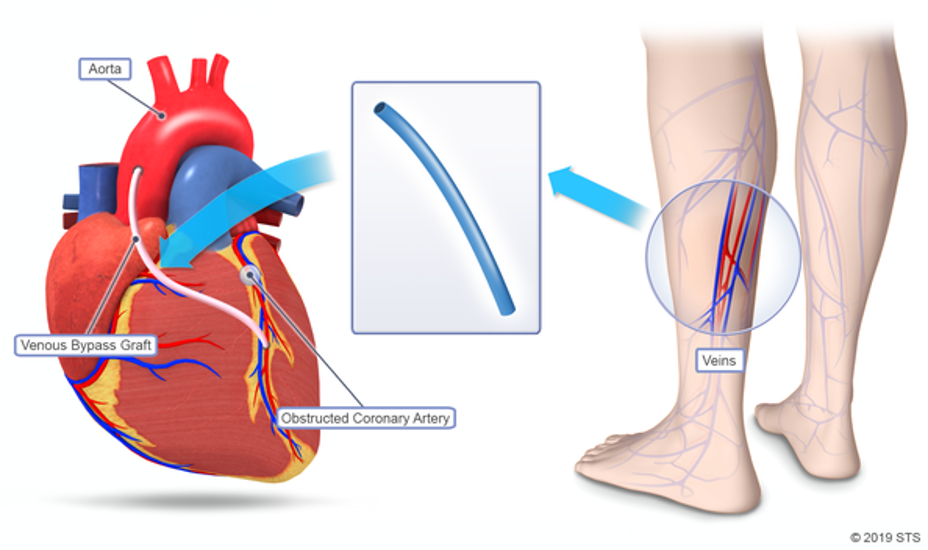
Bypass graft: The internal mammary, radial, and, in rare cases, gastroepiploic arteries are used in arterial grafts. Beyond the stenosis or occlusion, the internal mammary is mobilized and anastomosed to the coronary artery. Through open or minimally invasive incisions, vein grafts are taken from the leg's long saphenous vein and anastomosed from the aorta to the coronary artery beyond the stenosis or occlusion.
Closure: The bypass circuit is turned off for the patient, enabling the heart to fill and begin contracting again. Sinus rhythm either spontaneously resumes with systemic rewarming or is restored via cardioversion. All cannulas are removed once adequate cardiac output, and protamine is given to reverse heparin. Two sizable thoracostomy drains are placed into the chest cavity and pericardium, and temporary pacing wires are put into the atrium and/or ventricles. The skin is closed and the sternum is sealed with broken steel wires.
Complications
Stroke and neurocognitive impairment, myocardial infarction during surgery, transient anomalies in conduction and arrhythmias (such as atrial fibrillation), pericardial effusion/tamponade, hemorrhage, mediastinitis, infection from a sternal wound, renal failure, and mortality.
Prognosis
A 2-3.5% operational mortality rate. Venous grafts show a 50–60% 10-year patency, compared to 90% for left internal mammary artery grafts. When CABG is contrasted with percutaneous coronary intervention, it has demonstrated a decreased requirement for revascularization and an improved prognosis for patients with diabetes who are older than 65.
Indications
Triple coronary vessel disease, left main stem coronary artery disease, and two coronary vessel disease with a proximal left anterior descending artery lesion are the three primary anatomical reasons for CABG.
In these patients, CABG reduces angina and increases long-term survival.
Anatomy
After emerging from the ascending aorta, the right coronary artery passes anteriorly between the right auricle and the pulmonary trunk before descending via the atrioventricular groove.
It passes posteriorly and anastomoses with the left coronary artery at the inferior heart boundary.
The ascending aorta gives rise to the left coronary artery, which splits into the left anterior descending and left circumflex arteries in the atrioventricular groove after passing posteriorly between the pulmonary trunk and the left auricle. The internal mammary artery originates from the subclavian artery and descends behind the costal cartilages along the pleura. It finishes at the sixth intercostal gap, when it splits into the musculophrenic and superior epigastric arteries.
Investigational studies
Prior to surgery: ECG, echocardiography, coronary angiography, and thallium perfusion scintigraphy. Bloods: crossmatch, clotting, U&Es, and FBC. general evaluation of anesthesia.
Close observation in an ITU setting following surgery. meticulous follow-up.
Actions
A median sternotomy was made. The heart, coronary vessels, and large vessels are exposed and examined during pericardial dissection. Nowadays, less invasive thoracotomy incisions are made in an effort to lessen the morbidity associated with sternotomy.
"On Pump" CABG: Cardiopulmonary bypass machines are utilized during cardiac surgery to oxygenate and circulate blood. Perfusionists operate these machines. Blood is taken out of the right atrium and redirected into the ascending aorta via a venous cannula, causing systemic hypothermia and the administration of IV heparin. The heart is given a cardioplegic solution to cause a hypothermic cardioplegic arrest so that surgery can be done.
"Off pump" CABG: The heart is allowed to continue beating by applying tissue stabilisers, which are devices, to the surgical site.
Bypass graft: The internal mammary, radial, and, in rare cases, gastroepiploic arteries are used in arterial grafts. Beyond the stenosis or occlusion, the internal mammary is mobilized and anastomosed to the coronary artery. Through open or minimally invasive incisions, vein grafts are taken from the leg's long saphenous vein and anastomosed from the aorta to the coronary artery beyond the stenosis or occlusion.
Closure: The bypass circuit is turned off for the patient, enabling the heart to fill and begin contracting again. Sinus rhythm either spontaneously resumes with systemic rewarming or is restored via cardioversion. All cannulas are removed once adequate cardiac output, and protamine is given to reverse heparin. Two sizable thoracostomy drains are placed into the chest cavity and pericardium, and temporary pacing wires are put into the atrium and/or ventricles. The skin is closed and the sternum is sealed with broken steel wires.
Complications
Stroke and neurocognitive impairment, myocardial infarction during surgery, transient anomalies in conduction and arrhythmias (such as atrial fibrillation), pericardial effusion/tamponade, hemorrhage, mediastinitis, infection from a sternal wound, renal failure, and mortality.
Prognosis
A 2-3.5% operational mortality rate. Venous grafts show a 50–60% 10-year patency, compared to 90% for left internal mammary artery grafts. When CABG is contrasted with percutaneous coronary intervention, it has demonstrated a decreased requirement for revascularization and an improved prognosis for patients with diabetes who are older than 65.
0 Comments
