- Published on
Surgery - Diverticular Disease
Introduction
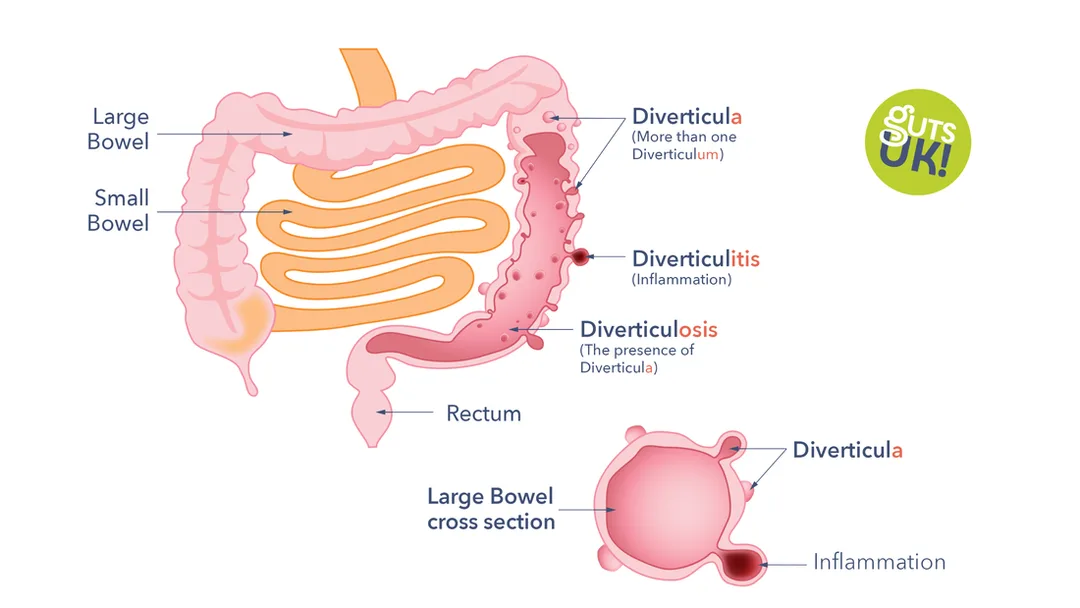
Diverticulae, or outpouchings of the colonic mucosa and submucosa through the large bowel's muscular wall, are indicative of diverticulosis.
Disease connected with diverticulitis: Diverticulitis linked to complications such as bleeding, infection, and fistulas.
Acute inflammation and infection of the colonic diverticulae is known as diverticulitis.
Classification of acute diverticulitis by Hinchey: Ia is phlegmon, II and III are localized abscesses, IV is faecal peritonitis, and VI is a perforation with purulent peritonitis.
Etiology
Loss of stool mass is a result of a low-fiber diet. High colonic intraluminal pressures are therefore required to force the stool through the muscularis, which causes the mucosa and submucosa to herniate.
Epidemiology
Colonic diverticulae are common (60 percent of persons in industrialized nations will acquire them), rare (less than 40 years). Diverticulae with a right slant are more prevalent in Asia.
History
80–90% of the time asymptomatic. PR bleeding, diverticulitis (usually), lower abdomen pain or the left iliac fossa, and fever are among the complications. Diverticular fistulation into the bladder causing recurrent UTIs, pneumaturia, and faecaluria.
Examination
Diverticulitis: sore abdomen; if a perforation has occurred, symptoms of localized or widespread peritonitis may be present.
Pathogenesis
Diverticulae can be right-sided, but they are most frequently found in the descending colon and sigmoid.
not present in the rectum. Herniated mucosa and submucosa via the muscularis, especially at areas of nutritional artery penetration, comprise diverticulae. The creation of fistulation or strictures, bacterial overgrowth, toxins, mucosal damage, diverticulitis, perforation, pericolic phlegmon, abscess, and ulceration can all result from proposed diverticular blockage caused by inspissated feces.
Investigations
Blood: FBC, elevated WCC and elevated CRP in cases of diverticulitis; if bleeding, examine coagulation and crossmatch.
Barium enema (air contrast): Shows pseudo-hypertrophy of circular muscle by displaying diverticulae with a sawtooth lumen appearance (should not be conducted in acute setting since there is a danger of perforation).
Flexible sigmoidoscopy and colonoscopy: This allows for the exclusion of additional pathologies, such as polyps or tumors, and the observation of diverticulae.
Check for signs of diverticular disease and consequences with a CT scan in an urgent situation.
Management
High-fibre diet (20–30 g/day): asymptomatic. Research is being done to see if probiotics and anti-inflammatories like mesalazine can stop diverticulitis from flare-ups repeatedly.
GI bleeding: IV rehydration and, if required, blood transfusions are frequently used as conservative measures to treat PR bleeding. embolization, angiography, and, if necessary, surgery.
IV antibiotics, fluid rehydration, and bowel rest are the treatments for diverticulitis. Drains placed radiologically may be used to treat localized collections or abscesses.
Surgery: May be required if there are repeated episodes or if complications like perforation and peritonitis arise. There are two types of surgery: open and laparoscopic.
Open: One-stage resection and anastomosis (leak risk) defuncting stoma; Hartmann's operation (resection and stoma). Laparoscopic drainage, peritoneal lavage, and drain insertion have shown promise in recent years.
Complications
Haemorrhage, fistula formation (bladder, small intestine, vagina), colonic blockage, diverticulitis, pericolic abscess, perforation, faecal peritonitis, and so on.
Prognosis
Between ten and twenty-five percent of people will get diverticulitis at least once. Thirty percent of them will have another incident.
Introduction
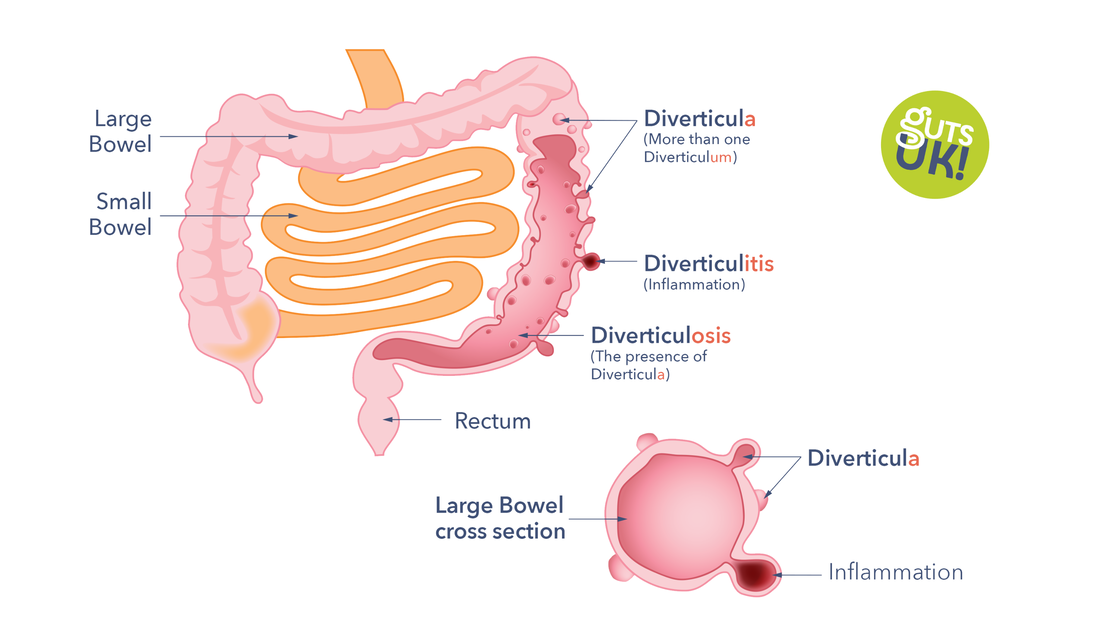
Diverticulae, or outpouchings of the colonic mucosa and submucosa through the large bowel's muscular wall, are indicative of diverticulosis.
Disease connected with diverticulitis: Diverticulitis linked to complications such as bleeding, infection, and fistulas.
Acute inflammation and infection of the colonic diverticulae is known as diverticulitis.
Classification of acute diverticulitis by Hinchey: Ia is phlegmon, II and III are localized abscesses, IV is faecal peritonitis, and VI is a perforation with purulent peritonitis.
Etiology
Loss of stool mass is a result of a low-fiber diet. High colonic intraluminal pressures are therefore required to force the stool through the muscularis, which causes the mucosa and submucosa to herniate.
Epidemiology
Colonic diverticulae are common (60 percent of persons in industrialized nations will acquire them), rare (less than 40 years). Diverticulae with a right slant are more prevalent in Asia.
History
80–90% of the time asymptomatic. PR bleeding, diverticulitis (usually), lower abdomen pain or the left iliac fossa, and fever are among the complications. Diverticular fistulation into the bladder causing recurrent UTIs, pneumaturia, and faecaluria.
Examination
Diverticulitis: sore abdomen; if a perforation has occurred, symptoms of localized or widespread peritonitis may be present.
Pathogenesis
Diverticulae can be right-sided, but they are most frequently found in the descending colon and sigmoid.
not present in the rectum. Herniated mucosa and submucosa via the muscularis, especially at areas of nutritional artery penetration, comprise diverticulae. The creation of fistulation or strictures, bacterial overgrowth, toxins, mucosal damage, diverticulitis, perforation, pericolic phlegmon, abscess, and ulceration can all result from proposed diverticular blockage caused by inspissated feces.
Investigations
Blood: FBC, elevated WCC and elevated CRP in cases of diverticulitis; if bleeding, examine coagulation and crossmatch.
Barium enema (air contrast): Shows pseudo-hypertrophy of circular muscle by displaying diverticulae with a sawtooth lumen appearance (should not be conducted in acute setting since there is a danger of perforation).
Flexible sigmoidoscopy and colonoscopy: This allows for the exclusion of additional pathologies, such as polyps or tumors, and the observation of diverticulae.
Check for signs of diverticular disease and consequences with a CT scan in an urgent situation.
Management
High-fibre diet (20–30 g/day): asymptomatic. Research is being done to see if probiotics and anti-inflammatories like mesalazine can stop diverticulitis from flare-ups repeatedly.
GI bleeding: IV rehydration and, if required, blood transfusions are frequently used as conservative measures to treat PR bleeding. embolization, angiography, and, if necessary, surgery.
IV antibiotics, fluid rehydration, and bowel rest are the treatments for diverticulitis. Drains placed radiologically may be used to treat localized collections or abscesses.
Surgery: May be required if there are repeated episodes or if complications like perforation and peritonitis arise. There are two types of surgery: open and laparoscopic.
Open: One-stage resection and anastomosis (leak risk) defuncting stoma; Hartmann's operation (resection and stoma). Laparoscopic drainage, peritoneal lavage, and drain insertion have shown promise in recent years.
Complications
Haemorrhage, fistula formation (bladder, small intestine, vagina), colonic blockage, diverticulitis, pericolic abscess, perforation, faecal peritonitis, and so on.
Prognosis
Between ten and twenty-five percent of people will get diverticulitis at least once. Thirty percent of them will have another incident.
0 Comments
