- Published on
Surgery - Esophageal Perforation
Introduction
rupture of the oesphogeal wall, frequently resulting in mediastinum contents spilling out.
Etiology
The Boerhaave syndrome is spontaneous. In the absence of underlying illness, barogenic disruption of the oesophageal wall is most frequently brought on by violent vomiting and sometimes strong Valsalva maneuvers, such as parturition or intense weightlifting.
Iatrogenic: During dilatation or upper gastrointestinal endoscopy, for example.
Trauma: foreign bodies, penetrating wounds, and infrequently blunt injuries.
Caustic: Consuming acid or alkali "lye" increases the risk of perforation and causes liquefactive or coagulative necrosis.
Epidemiology
Males > females (4: 1), a rare case of Boerhaave's condition.
History
abrupt, intense chest pain that usually follows a period of elevated intra-abdominal pressure and vomiting. It takes a great degree of suspicion.
Examination
The Mackler trinity, which includes vomiting, chest pain, and subcutaneous emphysema, includes tachypnea, tachycardia, and epigastric tenderness. Rarely does haematemesis occur.
Pathogenesis
In the distal oesophagus, spontaneous perforations typically manifest as a longitudinal tear that happens posterolaterally. Gastric contents are drawn into the mediastinum and pleural cavity by negative intrathoracic pressure, which results in chemical mediastinitis and quickly progresses to severe sepsis.
Ten to twenty percent are linked to underlying disorders of the oesophagus, such as infection, cancer, or peptic ulcer.
Investigational studies
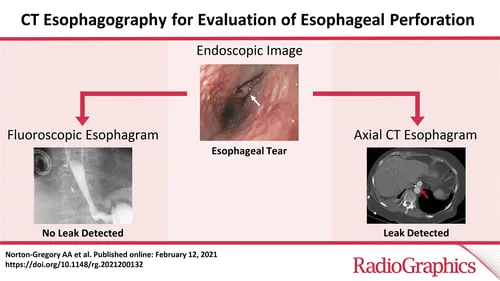
Imaging: Pleural effusion, air-fluid collections, pneumothorax, pneumediastinum, and subcutaneous emphysema can all be seen with a CXR or CT scan. Swallow a water-soluble contrast agent to identify leaks (10% false negatives).
Oesophagogastroscopy: Should only be carried out in a suitable facility by skilled endoscopists. able to verify the damage site, degree, and presence of any underlying pathology.
permits the nasogastric tube to be inserted for gastric drainage as well.
Management
Emergency: ABC resuscitation: oxygen, ventilation, and circulatory support; IV fluids; catheterization of the urinary tract; stringent fluid management; IV proton pump inhibitors; early intensivist review; interdisciplinary treatment; and close observation in an ICU or HDU.
Control of sepsis: no oral medication, starting broad-spectrum antibiotics and antifungal medications, maintaining adequate chest drainage, and continuing feeding. best treated in a dedicated oesophagogastric unit.
Non-operative management: Only in few instances with low contamination or cervical perforations, early detection, and limited harm. It is reported that some early perforations were clipped endoscopically.
Thoracotomy, devitalized oesophageal tissue, drainage, and debridement of contaminated area are the surgical procedures. Primary repair and reinforcement, such as flap pleura or intercostal muscle (which may fail and leak), repair over T-tube (which permits formation of a controlled oesophagocutaneous fistula), oesophageal resection with either immediate or delayed reconstruction (a major undertaking), and exclusion and diversion (which forms an oesophagostomy and requires reconstruction later) are among the available treatment options.
It is necessary to create a feeding jejunostomy for enteral feeding.
Complications
Subcutaneous emphysema, pleural effusion, severe sepsis, shock, multiple organ failure, and death are possible outcomes.
Prognosis
20% overall high death rate (up to 60% in cases of late presentations; 10% with early diagnosis and treatment).
Introduction
rupture of the oesphogeal wall, frequently resulting in mediastinum contents spilling out.
Etiology
The Boerhaave syndrome is spontaneous. In the absence of underlying illness, barogenic disruption of the oesophageal wall is most frequently brought on by violent vomiting and sometimes strong Valsalva maneuvers, such as parturition or intense weightlifting.
Iatrogenic: During dilatation or upper gastrointestinal endoscopy, for example.
Trauma: foreign bodies, penetrating wounds, and infrequently blunt injuries.
Caustic: Consuming acid or alkali "lye" increases the risk of perforation and causes liquefactive or coagulative necrosis.
Epidemiology
Males > females (4: 1), a rare case of Boerhaave's condition.
History
abrupt, intense chest pain that usually follows a period of elevated intra-abdominal pressure and vomiting. It takes a great degree of suspicion.
Examination
The Mackler trinity, which includes vomiting, chest pain, and subcutaneous emphysema, includes tachypnea, tachycardia, and epigastric tenderness. Rarely does haematemesis occur.
Pathogenesis
In the distal oesophagus, spontaneous perforations typically manifest as a longitudinal tear that happens posterolaterally. Gastric contents are drawn into the mediastinum and pleural cavity by negative intrathoracic pressure, which results in chemical mediastinitis and quickly progresses to severe sepsis.
Ten to twenty percent are linked to underlying disorders of the oesophagus, such as infection, cancer, or peptic ulcer.
Investigational studies
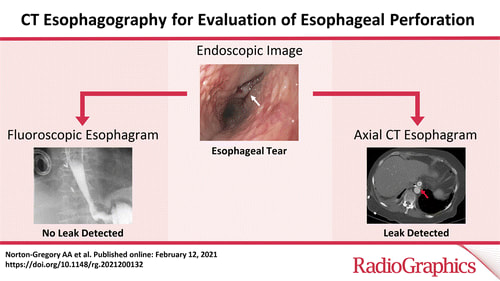
Imaging: Pleural effusion, air-fluid collections, pneumothorax, pneumediastinum, and subcutaneous emphysema can all be seen with a CXR or CT scan. Swallow a water-soluble contrast agent to identify leaks (10% false negatives).
Oesophagogastroscopy: Should only be carried out in a suitable facility by skilled endoscopists. able to verify the damage site, degree, and presence of any underlying pathology.
permits the nasogastric tube to be inserted for gastric drainage as well.
Management
Emergency: ABC resuscitation: oxygen, ventilation, and circulatory support; IV fluids; catheterization of the urinary tract; stringent fluid management; IV proton pump inhibitors; early intensivist review; interdisciplinary treatment; and close observation in an ICU or HDU.
Control of sepsis: no oral medication, starting broad-spectrum antibiotics and antifungal medications, maintaining adequate chest drainage, and continuing feeding. best treated in a dedicated oesophagogastric unit.
Non-operative management: Only in few instances with low contamination or cervical perforations, early detection, and limited harm. It is reported that some early perforations were clipped endoscopically.
Thoracotomy, devitalized oesophageal tissue, drainage, and debridement of contaminated area are the surgical procedures. Primary repair and reinforcement, such as flap pleura or intercostal muscle (which may fail and leak), repair over T-tube (which permits formation of a controlled oesophagocutaneous fistula), oesophageal resection with either immediate or delayed reconstruction (a major undertaking), and exclusion and diversion (which forms an oesophagostomy and requires reconstruction later) are among the available treatment options.
It is necessary to create a feeding jejunostomy for enteral feeding.
Complications
Subcutaneous emphysema, pleural effusion, severe sepsis, shock, multiple organ failure, and death are possible outcomes.
Prognosis
20% overall high death rate (up to 60% in cases of late presentations; 10% with early diagnosis and treatment).
0 Comments
