- Published on
Surgery - Femoral Hernia
Introduction
the unusual outgrowth of a peritoneal sac via the femoral canal, frequently containing contents from the abdomen.
Etiology
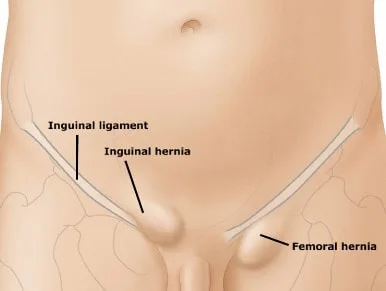
The structure of the femoral canal, which has four distinct and impervious borders, is the predisposing factor. These limits are the inguinal ligament anteriorly, the lacunar ligament medially, the pectineal (Cooper's) ligament and pubic bone posteriorly, and the femoral vein laterally. Usually, the canal simply contains a lymph node (Cloquet's node) and loose connective tissue.
R isk Factors
Women's femoral canals are wider due to the larger angle between the inguinal ligament and the pectineal portion of the pubic bone. Increased intra-abdominal pressure, such as from coughing or straining because of constipation or prostatism, increases the risk of hernia formation.
Epidemiology
25 times less frequent than inguinal hernias, with a female to male ratio of 4:1.
H HISTORY
Show up with a possible discomfort-causing lump or bulge in the groin. Femoral hernias frequently go undiagnosed until they become strangulated or obstructed because of their tiny size and tight necks. Up to 80% of cases of femoral hernias present as emergencies with pain, distention of the abdomen, nausea, and vomiting.
Examination
Upon close examination, a swelling beneath and to the side of the pubic tubercle will be visible in the groin (but if it is significant, it may also spread up and across the inguinal ligament). The cough impulse above the inguinal ring is absent. The hernia may be extremely sensitive if the victim is imprisoned or strangled. stomach distension and tinkling bowel noises if obstructed.
Differentials include femoral aneurysm, groin or psoas abscess, hydrocoele or lipoma of the spermatic cord (in men), inguinal hernia, lymphadenopathy, and saphaena varix.
Investigational studies
Blood: ABG (for metabolic acidosis in intestinal ischaemia), FBC, U&Es, coagulation, G&S.
Visualization: When a different diagnosis is suspected, an AXR may reveal intestinal blockage or USS; nevertheless, if an imprisoned hernia is suspected, surgery should not be postponed. Could be an unintentional discovery, like a CT scan. When a herniogram is suspected, it can be done electively.
Management
Emergency care includes resuscitation with electrolyte balance correction and hydration, implantation of an NG tube in the event of vomiting, administration of antibiotics in the event of sepsis, and surgical repair as the last resort.
Surgery: The basic steps are to dissect the sac, examine and reduce its contents, remove the sac, and repair the defect. Typically, this is done by approximating the pectineal and inguinal ligaments with non-absorbable sutures (a procedure known as Cooper's ligament repair). An alternative is to insert a mesh plug into the femoral canal without using any tension.
It is possible to perform laparoscopic mesh repair using TAPP or TEP techniques. Three primary methods are available for open surgery:
1. Low transverse incision over hernia (Lockwood) (elective surgery).
2. Transinguinal (Lotheissen) incision via the transversalis fascia, inguinal canal, external oblique, and above and parallel to the inguinal ligament (may have a greater recurrence rate).
3. The high (McEvedy) technique involves splitting the transversalis fascia, opening the rectus sheath, retracting the rectus medially, and making an oblique, paramedian, or unilateral Pfannenstiel incision to reveal the femoral canal. If strangulation is suspected, this is used. The sac's contents are examined after it is opened. If they are viable, they are decreased, and if nonviable bowel is present, it is removed (this may require resection if a high approach is not taken).
Complications
Femoral hernias frequently strangulate, which can cause gangrene, ischaemia, and intestinal blockage. Surgical resection may be required in some cases.
Surgery: Bleeding (an anomalous obturator artery may be wounded if the lacunar ligament is cut to enlarge the canal); there is a chance that the femoral vein may narrow during surgery, which increases the risk of seroma, infection, and venous thrombosis.
When timely and adequate surgery is performed, the prognosis for is generally good. Recurrence following repair is uncommon (<3%).
Introduction
the unusual outgrowth of a peritoneal sac via the femoral canal, frequently containing contents from the abdomen.
Etiology
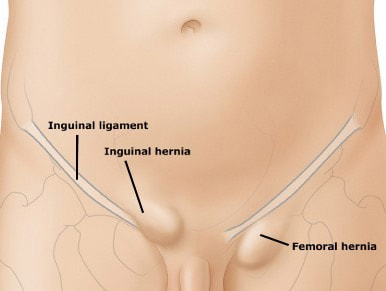
The structure of the femoral canal, which has four distinct and impervious borders, is the predisposing factor. These limits are the inguinal ligament anteriorly, the lacunar ligament medially, the pectineal (Cooper's) ligament and pubic bone posteriorly, and the femoral vein laterally. Usually, the canal simply contains a lymph node (Cloquet's node) and loose connective tissue.
R isk Factors
Women's femoral canals are wider due to the larger angle between the inguinal ligament and the pectineal portion of the pubic bone. Increased intra-abdominal pressure, such as from coughing or straining because of constipation or prostatism, increases the risk of hernia formation.
Epidemiology
25 times less frequent than inguinal hernias, with a female to male ratio of 4:1.
H HISTORY
Show up with a possible discomfort-causing lump or bulge in the groin. Femoral hernias frequently go undiagnosed until they become strangulated or obstructed because of their tiny size and tight necks. Up to 80% of cases of femoral hernias present as emergencies with pain, distention of the abdomen, nausea, and vomiting.
Examination
Upon close examination, a swelling beneath and to the side of the pubic tubercle will be visible in the groin (but if it is significant, it may also spread up and across the inguinal ligament). The cough impulse above the inguinal ring is absent. The hernia may be extremely sensitive if the victim is imprisoned or strangled. stomach distension and tinkling bowel noises if obstructed.
Differentials include femoral aneurysm, groin or psoas abscess, hydrocoele or lipoma of the spermatic cord (in men), inguinal hernia, lymphadenopathy, and saphaena varix.
Investigational studies
Blood: ABG (for metabolic acidosis in intestinal ischaemia), FBC, U&Es, coagulation, G&S.
Visualization: When a different diagnosis is suspected, an AXR may reveal intestinal blockage or USS; nevertheless, if an imprisoned hernia is suspected, surgery should not be postponed. Could be an unintentional discovery, like a CT scan. When a herniogram is suspected, it can be done electively.
Management
Emergency care includes resuscitation with electrolyte balance correction and hydration, implantation of an NG tube in the event of vomiting, administration of antibiotics in the event of sepsis, and surgical repair as the last resort.
Surgery: The basic steps are to dissect the sac, examine and reduce its contents, remove the sac, and repair the defect. Typically, this is done by approximating the pectineal and inguinal ligaments with non-absorbable sutures (a procedure known as Cooper's ligament repair). An alternative is to insert a mesh plug into the femoral canal without using any tension.
It is possible to perform laparoscopic mesh repair using TAPP or TEP techniques. Three primary methods are available for open surgery:
1. Low transverse incision over hernia (Lockwood) (elective surgery).
2. Transinguinal (Lotheissen) incision via the transversalis fascia, inguinal canal, external oblique, and above and parallel to the inguinal ligament (may have a greater recurrence rate).
3. The high (McEvedy) technique involves splitting the transversalis fascia, opening the rectus sheath, retracting the rectus medially, and making an oblique, paramedian, or unilateral Pfannenstiel incision to reveal the femoral canal. If strangulation is suspected, this is used. The sac's contents are examined after it is opened. If they are viable, they are decreased, and if nonviable bowel is present, it is removed (this may require resection if a high approach is not taken).
Complications
Femoral hernias frequently strangulate, which can cause gangrene, ischaemia, and intestinal blockage. Surgical resection may be required in some cases.
Surgery: Bleeding (an anomalous obturator artery may be wounded if the lacunar ligament is cut to enlarge the canal); there is a chance that the femoral vein may narrow during surgery, which increases the risk of seroma, infection, and venous thrombosis.
When timely and adequate surgery is performed, the prognosis for is generally good. Recurrence following repair is uncommon (<3%).
0 Comments
