- Published on
Surgery - Gallbladder Cancer
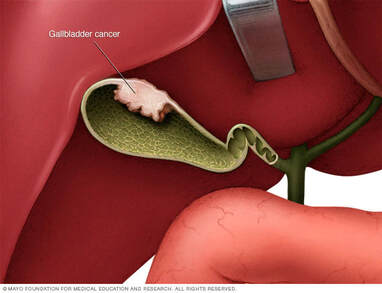
Introduction
Gallbladder-related malignancy.
Etiology
Just 0.3–3% of people with stones will go on to develop gallstone disease, which affects 80% of patients. a "porcelain gallbladder," so named due to up to 60% mural calcification.
abnormal pancreaticobiliary architecture and gallbladder polyps (>10mm).
Epidemiology
The most frequent gastrointestinal cancer, ranking fifth in frequency, usually affects those over 65. The ratio of women to men is 2-3:1.
History
Early detection could be found during a gallstone disease investigation. When there are symptoms, such pain, loss of appetite, and fullness in the abdomen, the illness has frequently progressed.
Examination
There can be a palpable lump in the right upper quadrant. indicators of a weight loss. a yellowish hue.
Pathogenesis
Adenocarcinomas account for 90% of cases, squamous carcinomas for 5%, and anaplastic carcinomas for 5%.
induration, thickening, or mass in the neck (5%), body (30%), or fundus (60%).
Investigational studies
Ultrasound: 85% sensitivity; may reveal thickness of the gallbladder wall, polyp or mass; color Doppler may increase specificity.
MRI, CT, MRA, and MRCP: To evaluate the tumor and look for metastases.
Other: laparoscopy, ERCP or PTC in cases of biliary blockage, and FDG-PET.
Cancer markers: CEA, CA19-9, and CA125 may exhibit elevated levels.
Management
Simple cholecystectomy for tumors limited to the mucosa or submucosa (T1a) is the surgical procedure.
Radical cholecystectomy with hepatic wedge resection (segments IV, V, at least 3 cm in depth), cystic duct resection, and regional lymph node resection are recommended for tumors penetrating the muscularis. A Roux-en-Y hepaticojejunostomy may be used to resect the common bile duct and restore biliary-enteric continuity in the event that pericholedochal nodes are affected.
Radiation therapy or chemotherapy: Certain agents exhibit partial reactions, such as 5-fluorouracil.
There is also radiotherapy.
Palliative: Percutaneous or endoscopic stenting can be used to treat obstructive jaundice. One of the main concerns is pain reduction, which can be achieved with chemical splanchnicectomy or percutaneous celiac nerve block. reacts poorly to radiation and chemotherapy.
Complications
Duodenal blockage, discomfort, and obstructive jaundice.
Spread: Lymphatic spread into the cystic, pancreaticoduodenal, celiac, and periaortic nodes; local direct invasion into the hepatic bed (venous draining into segment IV).
Additionally typical is transperitoneal spread.
Prognosis
The prognosis is bad, with a 5-year survival rate of only 5% for all cases save those that are unintentionally discovered during cholecystectomy.
Staging: TNM is correlated with prognosis based on invasion depth.
Introduction
Gallbladder-related malignancy.
Etiology
Just 0.3–3% of people with stones will go on to develop gallstone disease, which affects 80% of patients. a "porcelain gallbladder," so named due to up to 60% mural calcification.
abnormal pancreaticobiliary architecture and gallbladder polyps (>10mm).
Epidemiology
The most frequent gastrointestinal cancer, ranking fifth in frequency, usually affects those over 65. The ratio of women to men is 2-3:1.
History
Early detection could be found during a gallstone disease investigation. When there are symptoms, such pain, loss of appetite, and fullness in the abdomen, the illness has frequently progressed.
Examination
There can be a palpable lump in the right upper quadrant. indicators of a weight loss. a yellowish hue.
Pathogenesis
Adenocarcinomas account for 90% of cases, squamous carcinomas for 5%, and anaplastic carcinomas for 5%.
induration, thickening, or mass in the neck (5%), body (30%), or fundus (60%).
Investigational studies
Ultrasound: 85% sensitivity; may reveal thickness of the gallbladder wall, polyp or mass; color Doppler may increase specificity.
MRI, CT, MRA, and MRCP: To evaluate the tumor and look for metastases.
Other: laparoscopy, ERCP or PTC in cases of biliary blockage, and FDG-PET.
Cancer markers: CEA, CA19-9, and CA125 may exhibit elevated levels.
Management
Simple cholecystectomy for tumors limited to the mucosa or submucosa (T1a) is the surgical procedure.
Radical cholecystectomy with hepatic wedge resection (segments IV, V, at least 3 cm in depth), cystic duct resection, and regional lymph node resection are recommended for tumors penetrating the muscularis. A Roux-en-Y hepaticojejunostomy may be used to resect the common bile duct and restore biliary-enteric continuity in the event that pericholedochal nodes are affected.
Radiation therapy or chemotherapy: Certain agents exhibit partial reactions, such as 5-fluorouracil.
There is also radiotherapy.
Palliative: Percutaneous or endoscopic stenting can be used to treat obstructive jaundice. One of the main concerns is pain reduction, which can be achieved with chemical splanchnicectomy or percutaneous celiac nerve block. reacts poorly to radiation and chemotherapy.
Complications
Duodenal blockage, discomfort, and obstructive jaundice.
Spread: Lymphatic spread into the cystic, pancreaticoduodenal, celiac, and periaortic nodes; local direct invasion into the hepatic bed (venous draining into segment IV).
Additionally typical is transperitoneal spread.
Prognosis
The prognosis is bad, with a 5-year survival rate of only 5% for all cases save those that are unintentionally discovered during cholecystectomy.
Staging: TNM is correlated with prognosis based on invasion depth.

0 Comments
