- Published on
Surgery - Gallstones
Introduction
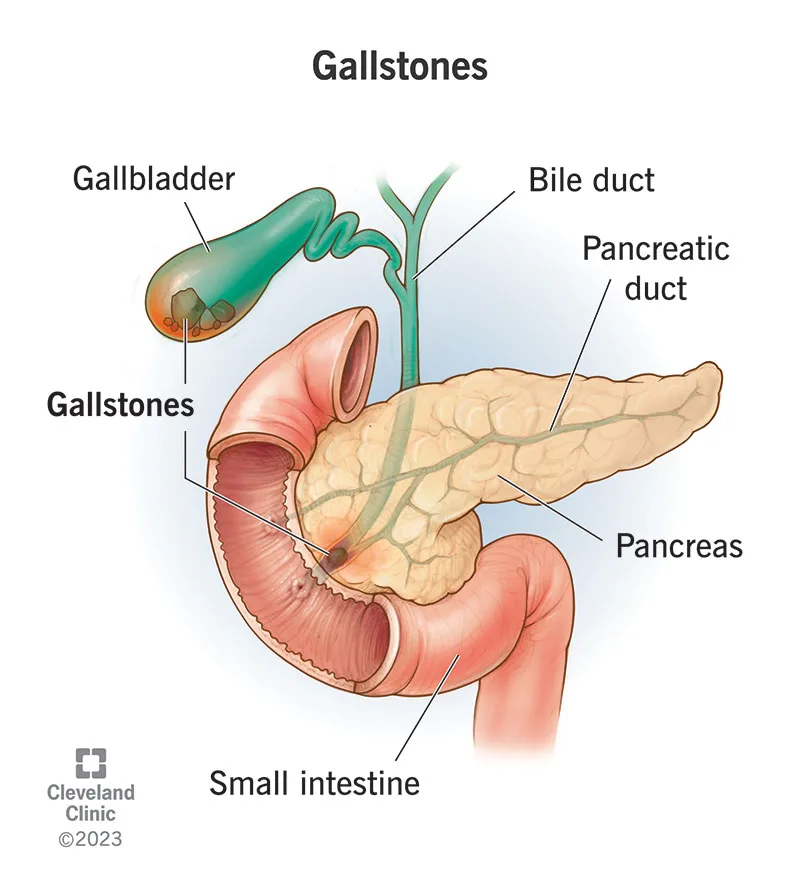
Development of stones in the gallbladder.
Etiology
Blended stones: comprise 80% protein, phosphate, calcium bilirubinate, and cholesterol.
associated with advanced age, female gender, obesity, parenteral nutrition, medications (OCP, octreotide), family history, ethnicity (e.g., Pima Indians), disruption of the enterohepatic recirculation of bile salts (e.g., Crohn's disease), and terminal ileal resection.
10% of stones are pure cholesterol. comparable relationships with mixed stones.
10% of pigment stones: Brown stones caused by bile duct infection by the liver fluke Clonorchis sinensis, and black stones composed of calcium bilirubinate, which raise bilirubin secondary to hemolytic illnesses such as sickle cell and cirrhosis.
Epidemiology
Quite frequent (prevalence of 10% in the UK), more prevalent as one ages, with 3 times as many females in the younger population but an equal sex ratio beyond 65. In the UK, 50,000 cholecystectomies are done each year.
History
Asymptomatic (90%): discovered by chance.
Biliary colic: Constant, intense pain in the right upper quadrant or epigastric area that develops suddenly. May radiate to the right scapula; heavy meals are frequently the cause of this. may be linked to vomiting and nausea.
Acute cholecystitis: fever, protracted upper abdominal pain, and systemic illness in the patient that may radiate to the right shoulder (diaphragmatic irritation).
Ascending cholangitis: Charcot's triad, which traditionally correlates right upper quadrant discomfort, jaundice, and rigors. It is referred to as Reynolds' pentad if it is accompanied by hypotension and disorientation.
Examination
Epigastric or right upper quadrant tenderness is a sign of biliary colic.
Right upper quadrant or epigastric discomfort, pyrexia, and tachycardia are signs of acute cholecystitis.
There may be a rebounding guard. A favorable Murphy's sign.
Ascending cholangitis: jaundice, pyrexia, and discomfort in the right upper quadrant.
Pathogenesis
The impaction of a gallstone in the cystic duct is the cause of biliary colic. resolves when the stone returns to the gallbladder or stays impacted, causing acute cholecystitis, mucosal oedema, and inflammation. Pathological alterations in chronic cholecystitis range from a shrunken, fibrosed gallbladder with transmural fibrosis to microscopic signs of persistent inflammation with the mucosa entering the muscle layer as Rokitansky–Aschoff sinuses.
Dystrophic calcification, which can lead to a porcelain gallbladder with a "risk of malignant transformation," happens infrequently.
Investigations
Blood: LFT ("AlkPhos, " bilirubin in ascending cholangitis), FBC ("WBC in cholecystitis or cholangitis"). Blood cultures, "transaminases," and amylase (risk of pancreatitis) may be present.
USS: Shows gallstones, which are audible shadows inside the gallbladder, as well as the thickness of the gallbladder wall. It can also check for the presence of biliary tree dilatation, which is a sign of obstruction. AXR: Radio-opaque gallstones occur seldom (10%) (Fig. 5).
Additional imaging options include CT scanning, MRCP, ERCP, or an erect CXR to rule out perforation as a differential diagnosis.
Management
Conservative: Limiting fat in the diet in cases with moderate biliary colic symptoms.
Medical: Oral dissolving therapy is only appropriate for a limited number of patients due to its poor effectiveness, slowness, and high recurrence rate. If the biliary colic is severe, a hospitalization, IV fluids with analgesics, and antiemetics may be necessary; antibiotics should be provided if there are signs of infection. It is advisable to suspect a localized abscess or empyema if symptoms do not improve or get worse. Using a pigtail catheter and cholecystostomy, this can be percutaneously emptied.
IV antibiotics and resuscitation are necessary if ascending cholangitis is present. ERCP or PTC should be used for immediate biliary drainage if there is blockage.
Surgical: Table cholangiogram with laparoscopic cholecystectomy (see Cholecystectomy). Should be carried out in an emergency situation either 72 hours after the commencement of ‘hot gallbladder symptoms or after a few weeks to let the inflammation to subside.
Complications
Within the gallbladder, stones: Gallbladder empyema or mucocoele, porcelain gallbladder, cholecystitis, biliary colic, and a rare propensity for gallbladder cancer.
The following conditions can result from stones outside the gallbladder: pancreatitis, ascending cholangitis, cholecystenteric fistula, gallstone ileus, Bouveret's syndrome (obstructive jaundice caused by gallstones obstructing the stomach outlet), and cholecystocholedochal fistula (also known as Mirizi's syndrome).
Bleeding, infection, bile leak, bile duct injury (0.3%), postcholecystectomy syndrome (permanent dyspeptic symptoms), and hernias are the following side effects of cholecystectomy.
Prognosis
Gallstones are generally benign and do not present with many difficulties (about 2% of gallstone sufferers experience symptoms each year). If present with symptoms, surgery is a useful intervention.
Introduction
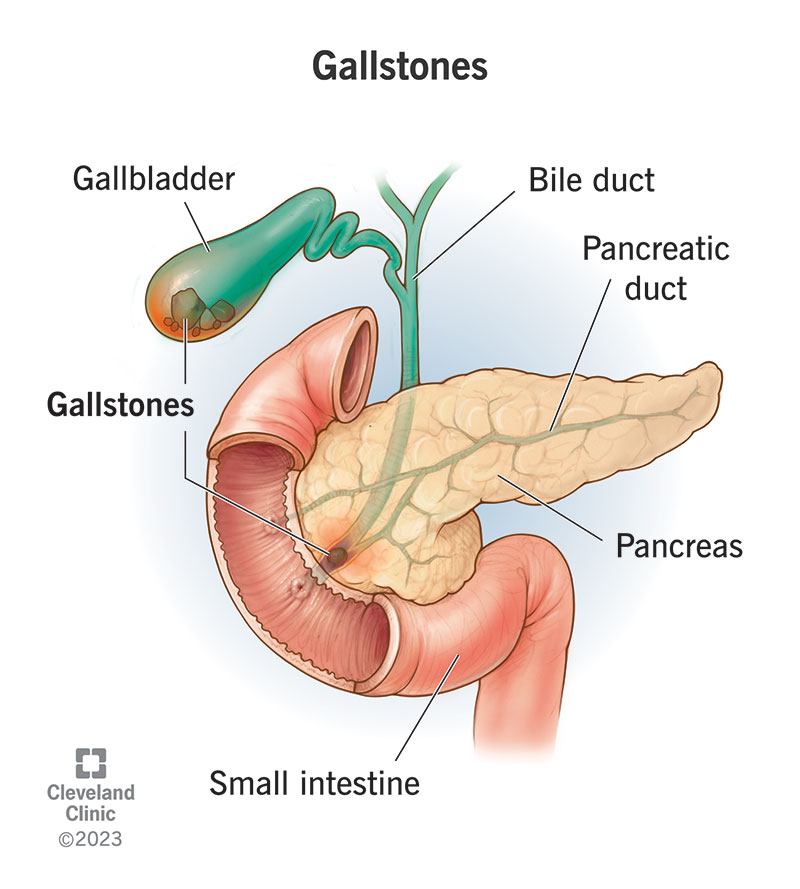
Development of stones in the gallbladder.
Etiology
Blended stones: comprise 80% protein, phosphate, calcium bilirubinate, and cholesterol.
associated with advanced age, female gender, obesity, parenteral nutrition, medications (OCP, octreotide), family history, ethnicity (e.g., Pima Indians), disruption of the enterohepatic recirculation of bile salts (e.g., Crohn's disease), and terminal ileal resection.
10% of stones are pure cholesterol. comparable relationships with mixed stones.
10% of pigment stones: Brown stones caused by bile duct infection by the liver fluke Clonorchis sinensis, and black stones composed of calcium bilirubinate, which raise bilirubin secondary to hemolytic illnesses such as sickle cell and cirrhosis.
Epidemiology
Quite frequent (prevalence of 10% in the UK), more prevalent as one ages, with 3 times as many females in the younger population but an equal sex ratio beyond 65. In the UK, 50,000 cholecystectomies are done each year.
History
Asymptomatic (90%): discovered by chance.
Biliary colic: Constant, intense pain in the right upper quadrant or epigastric area that develops suddenly. May radiate to the right scapula; heavy meals are frequently the cause of this. may be linked to vomiting and nausea.
Acute cholecystitis: fever, protracted upper abdominal pain, and systemic illness in the patient that may radiate to the right shoulder (diaphragmatic irritation).
Ascending cholangitis: Charcot's triad, which traditionally correlates right upper quadrant discomfort, jaundice, and rigors. It is referred to as Reynolds' pentad if it is accompanied by hypotension and disorientation.
Examination
Epigastric or right upper quadrant tenderness is a sign of biliary colic.
Right upper quadrant or epigastric discomfort, pyrexia, and tachycardia are signs of acute cholecystitis.
There may be a rebounding guard. A favorable Murphy's sign.
Ascending cholangitis: jaundice, pyrexia, and discomfort in the right upper quadrant.
Pathogenesis
The impaction of a gallstone in the cystic duct is the cause of biliary colic. resolves when the stone returns to the gallbladder or stays impacted, causing acute cholecystitis, mucosal oedema, and inflammation. Pathological alterations in chronic cholecystitis range from a shrunken, fibrosed gallbladder with transmural fibrosis to microscopic signs of persistent inflammation with the mucosa entering the muscle layer as Rokitansky–Aschoff sinuses.
Dystrophic calcification, which can lead to a porcelain gallbladder with a "risk of malignant transformation," happens infrequently.
Investigations
Blood: LFT ("AlkPhos, " bilirubin in ascending cholangitis), FBC ("WBC in cholecystitis or cholangitis"). Blood cultures, "transaminases," and amylase (risk of pancreatitis) may be present.
USS: Shows gallstones, which are audible shadows inside the gallbladder, as well as the thickness of the gallbladder wall. It can also check for the presence of biliary tree dilatation, which is a sign of obstruction. AXR: Radio-opaque gallstones occur seldom (10%) (Fig. 5).
Additional imaging options include CT scanning, MRCP, ERCP, or an erect CXR to rule out perforation as a differential diagnosis.
Management
Conservative: Limiting fat in the diet in cases with moderate biliary colic symptoms.
Medical: Oral dissolving therapy is only appropriate for a limited number of patients due to its poor effectiveness, slowness, and high recurrence rate. If the biliary colic is severe, a hospitalization, IV fluids with analgesics, and antiemetics may be necessary; antibiotics should be provided if there are signs of infection. It is advisable to suspect a localized abscess or empyema if symptoms do not improve or get worse. Using a pigtail catheter and cholecystostomy, this can be percutaneously emptied.
IV antibiotics and resuscitation are necessary if ascending cholangitis is present. ERCP or PTC should be used for immediate biliary drainage if there is blockage.
Surgical: Table cholangiogram with laparoscopic cholecystectomy (see Cholecystectomy). Should be carried out in an emergency situation either 72 hours after the commencement of ‘hot gallbladder symptoms or after a few weeks to let the inflammation to subside.
Complications
Within the gallbladder, stones: Gallbladder empyema or mucocoele, porcelain gallbladder, cholecystitis, biliary colic, and a rare propensity for gallbladder cancer.
The following conditions can result from stones outside the gallbladder: pancreatitis, ascending cholangitis, cholecystenteric fistula, gallstone ileus, Bouveret's syndrome (obstructive jaundice caused by gallstones obstructing the stomach outlet), and cholecystocholedochal fistula (also known as Mirizi's syndrome).
Bleeding, infection, bile leak, bile duct injury (0.3%), postcholecystectomy syndrome (permanent dyspeptic symptoms), and hernias are the following side effects of cholecystectomy.
Prognosis
Gallstones are generally benign and do not present with many difficulties (about 2% of gallstone sufferers experience symptoms each year). If present with symptoms, surgery is a useful intervention.


0 Comments
