- Published on
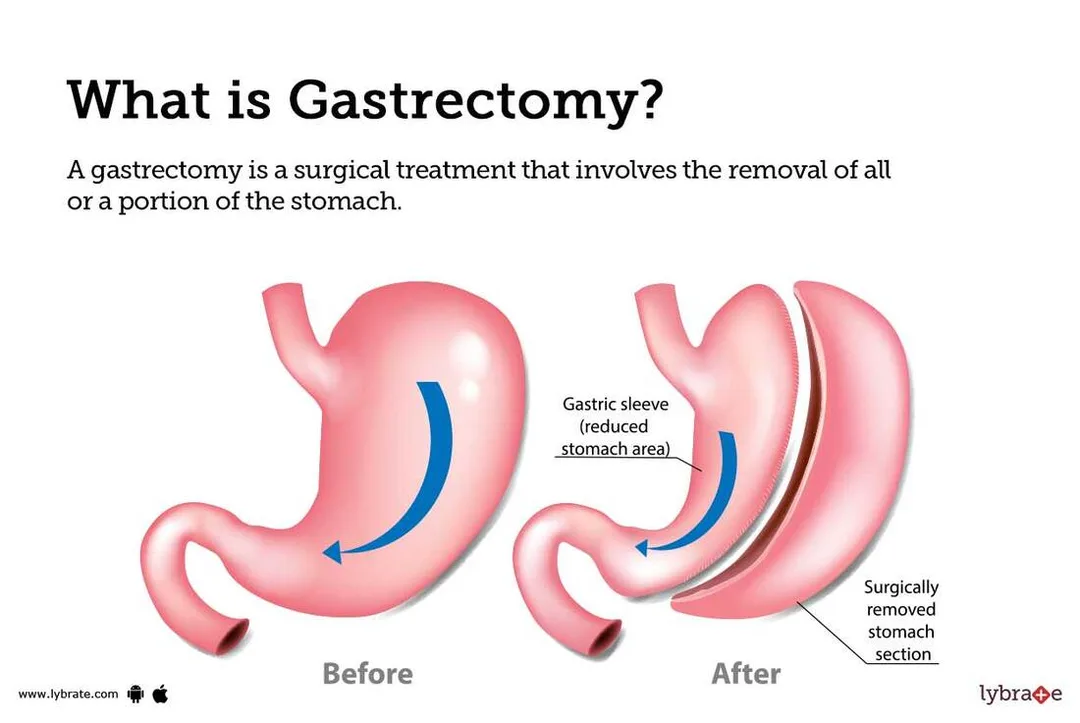
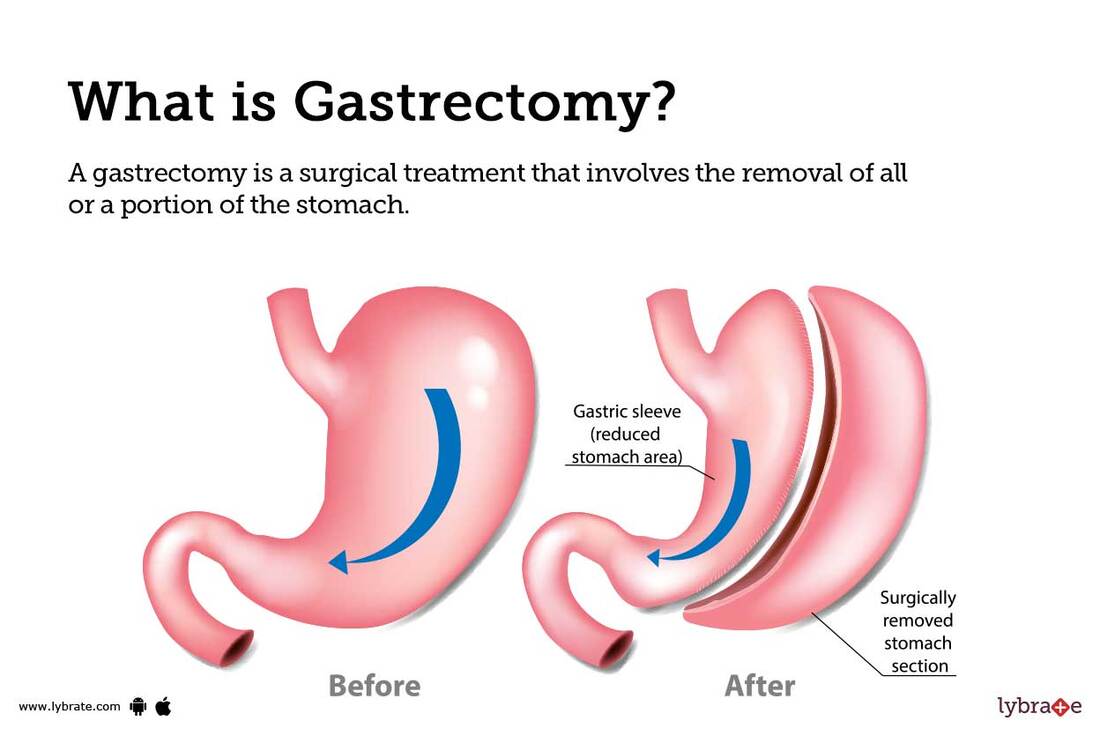
Surgery - Gastrectomies
Indications
Elective: Severe peptic ulcer illness, benign and malignant tumors.
Emergency: bleeding or puncture that cannot be stopped with local anesthesia; stomach necrosis, such as that resulting from gastric volvulus.
Anatomy
The stomach has minor and greater curvatures and is separated into the cardia, fundus, body, antrum, and pylorus.
Vascular: The stomach is supplied by the gastroepiploic, short, left, and right gastric arteries (which are often derived from the hepatic artery). The celiac axis has all of these branches. The portal vein receives venous drainage from matching veins. The location of portal-systemic anastomosis is the gastro-oesophageal junction.
The lymphatic system is made up of several lymph nodes that follow arteries and give rise to lymph nodes in the stomach, colon, pancreaticoduodenal, splenic, gastroepiploic, portahepatic, paraoesophageal, and para-aortic regions.
nerve supply Terminal branches of the left and right vagus nerves are parasympathetic.
T6–T9 segments that travel via the celiac plexus and are dispersed across the larger splanchnic nerve are considered sympathetic.
Investigational studies
Imaging: If a perforation is suspected, perform an emergency AXR and CXR (erect). CT scan: For determining resectibility and staging.
Endoscopy: endoscopic ultrasound tumor staging, optical generalization for biopsies.
Pre-op: FBC, U&Es, clotting, and crossmatch are the appropriate blood types. Before a final procedure, a staging laparoscopy may be carried out on stomach tumors to determine their resectibility.
After surgery: IV fluids, urine catheter, and NG or nasojejunal tube. prevention of DVT. Parenteral feeding could be required in the first several days following surgery.
Actions
Cutting: Open: Usually a diagonal "sabreslash" incision or an upper midline incision. increased the amount of laparoscopic procedures.
Gastrectomy types:
Subtotal distal gastrectomy (Billroth I). After reconstruction, the proximal stomach's smaller curve is anastomosed to the duodenum. less frequently carried out these days.
Polya partial gastrectomy, or Billroth II: A gastrojejunostomy is created when the proximal gastric remnant is anastomosed to the jejunum following distal stomach resection. A blind loop is created by the oversewing of the duodenum at its proximal end. Bile reflux is a possible side effect of Billroths I and II.
Roux-en-Y partial gastrectomy: The jejunum is divided after the distal stomach is removed, with the proximal jejunum being anastomosed further along the jejunum to form a Roux loop and the distal end being anastomosed to the gastric remnant.
Complete gastrectomy: The entire stomach is removed, and typically a Roux-en-Y loop is used to anastomose the distal oesophagus to the jejunum in order to restore intestinal continuity. The terms "D1 or D2 gastrectomies" refer to the radicality of lymph node clearance. While D2 entails more radical nodal clearance (coeliac, splenic, and common hepatic nodes), D1 requires clearing the N1 or first tier of perigastric nodes. It is possible to do distal pancreatectomy and splenectomy, although doing so raises the rate of operational death (from 4% to 15%) without improving cancer survival.
Oesophagogastrectomy in two phases: carried out for oesophageal or gastrooesophageal junction tumors. The chest phase includes oesophagectomy, lymphadectomy, gastric pull up into the chest, and construction of a gastric tube conduit after abdominal gastric mobilization and lymphadenectomy.
Complications
Early symptoms include bleeding, fistula formation, pancreatitis, anastomotic leak, infection, and duodenal stump leakage.
Long-range: Vitamin B12 deficiency, dumping syndromes (early and late), weight loss, reflux, diarrhea, stomal ulceration, blind loop syndrome, anemia, and metabolic bone disease
Indications
Elective: Severe peptic ulcer illness, benign and malignant tumors.
Emergency: bleeding or puncture that cannot be stopped with local anesthesia; stomach necrosis, such as that resulting from gastric volvulus.
Anatomy
The stomach has minor and greater curvatures and is separated into the cardia, fundus, body, antrum, and pylorus.
Vascular: The stomach is supplied by the gastroepiploic, short, left, and right gastric arteries (which are often derived from the hepatic artery). The celiac axis has all of these branches. The portal vein receives venous drainage from matching veins. The location of portal-systemic anastomosis is the gastro-oesophageal junction.
The lymphatic system is made up of several lymph nodes that follow arteries and give rise to lymph nodes in the stomach, colon, pancreaticoduodenal, splenic, gastroepiploic, portahepatic, paraoesophageal, and para-aortic regions.
nerve supply Terminal branches of the left and right vagus nerves are parasympathetic.
T6–T9 segments that travel via the celiac plexus and are dispersed across the larger splanchnic nerve are considered sympathetic.
Investigational studies
Imaging: If a perforation is suspected, perform an emergency AXR and CXR (erect). CT scan: For determining resectibility and staging.
Endoscopy: endoscopic ultrasound tumor staging, optical generalization for biopsies.
Pre-op: FBC, U&Es, clotting, and crossmatch are the appropriate blood types. Before a final procedure, a staging laparoscopy may be carried out on stomach tumors to determine their resectibility.
After surgery: IV fluids, urine catheter, and NG or nasojejunal tube. prevention of DVT. Parenteral feeding could be required in the first several days following surgery.
Actions
Cutting: Open: Usually a diagonal "sabreslash" incision or an upper midline incision. increased the amount of laparoscopic procedures.
Gastrectomy types:
Subtotal distal gastrectomy (Billroth I). After reconstruction, the proximal stomach's smaller curve is anastomosed to the duodenum. less frequently carried out these days.
Polya partial gastrectomy, or Billroth II: A gastrojejunostomy is created when the proximal gastric remnant is anastomosed to the jejunum following distal stomach resection. A blind loop is created by the oversewing of the duodenum at its proximal end. Bile reflux is a possible side effect of Billroths I and II.
Roux-en-Y partial gastrectomy: The jejunum is divided after the distal stomach is removed, with the proximal jejunum being anastomosed further along the jejunum to form a Roux loop and the distal end being anastomosed to the gastric remnant.
Complete gastrectomy: The entire stomach is removed, and typically a Roux-en-Y loop is used to anastomose the distal oesophagus to the jejunum in order to restore intestinal continuity. The terms "D1 or D2 gastrectomies" refer to the radicality of lymph node clearance. While D2 entails more radical nodal clearance (coeliac, splenic, and common hepatic nodes), D1 requires clearing the N1 or first tier of perigastric nodes. It is possible to do distal pancreatectomy and splenectomy, although doing so raises the rate of operational death (from 4% to 15%) without improving cancer survival.
Oesophagogastrectomy in two phases: carried out for oesophageal or gastrooesophageal junction tumors. The chest phase includes oesophagectomy, lymphadectomy, gastric pull up into the chest, and construction of a gastric tube conduit after abdominal gastric mobilization and lymphadenectomy.
Complications
Early symptoms include bleeding, fistula formation, pancreatitis, anastomotic leak, infection, and duodenal stump leakage.
Long-range: Vitamin B12 deficiency, dumping syndromes (early and late), weight loss, reflux, diarrhea, stomal ulceration, blind loop syndrome, anemia, and metabolic bone disease
0 Comments
