- Published on
Surgery -Ileus and Pseudo obstruction
Introduction
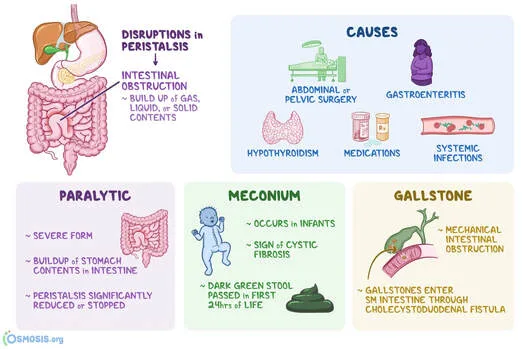
Blockage of the colon that is functional but does not have a mechanical source because of atony or abnormal peristalsis.
Etiology
Postoperative: Atonement of the bowel after intraabdominal surgery.
Metabolic conditions include liver failure, hypomagnesemia, hypokalaemia, ketoacidosis, and uraemia.
Response to an inflammatory disease, such as cholecystitis, is called infection or inflammation.
Chemical or bacterial diffuse peritonitis.
Pathology of the retroperitoneum: hemorrhage, pancreatitis.
Drugs: antipsychotics, anticholinergics, and opioids.
Scleroderma, multiple sclerosis, Parkinson's disease, and diabetes are examples of neuropathic illnesses.
Ogilvie's syndrome: Colonic pseudo-obstruction linked to polypharmacy, chronic illness, immobility, and long-term debility.
Epidemiology
depending on the cause, but a prevalent issue in people undergoing surgery. Acute colonic pseudoobstruction typically affects older people who have coexisting medical conditions.
History
Past events related to the cause, such as a recent operation. Constipation and inability to pass gas. stomach distension at first without discomfort, but later symptoms could resemble those of a real blockage.
Examination
stomach distension. There could be less or no bowel sounds. Soreness, potential problems, and/or peritonism. A rectal examination may reveal faecal impaction.
Investigations
in accordance with the aetiology and condition of the patient. Possible contents include:
FBC, U&Es, Mg2+, ESR, and CRP in blood.
Visualization: A CT scan, erect CXR and AXR, may reveal intestinal distension and faecal impaction.
>12 cm caecal diameter considerably increases the chance of perforation.A water-soluble contrast enema aids in distinguishing between an obstruction that is mechanical.
Managements
Depending on the aetiology, the following methods are frequently employed:
Nebulization by NG tube if vomiting, IV fluid replenishment, and correction of electrolyte imbalances (particularly hypokalaemia and hypomagnesaemia) are supportive measures. A flatus tube inserted could aid in decompression. Avoiding laxatives and medications that lower intestinal motility, particularly those that contain osmotic substances like lactulose.
Medical: Addressing the underlying issue, such as an infection. Prokinetic medications like metoclopramide and domperidone may be effective in treating chronic paralytic ileus in the absence of mechanical obstruction. If there is an acute colonic pseudoobstruction, IV neostigmine can be administered, but it must be well monitored due to the risk of hypotension, bradycardia, and brochospasm.
Endoscopic decompression: Has a 2% risk of perforation and can be useful in cases of colonic pseudo-obstruction.
Surgical: For severe morbidity and mortality, impending or actualized perforation. Decompression and stoma creation; in the event of complications, ileorectal anastamosis or segmental or subtotal colonic resection and exteriorization.
Complications
Bowel perforation, peritonitis, most frequently caecal (40% mortality).
Prognosis
Typically reacts to precautionary actions. Overall mortality from acute colonic pseudo-obstruction ranges from 25 to 31%.
Introduction
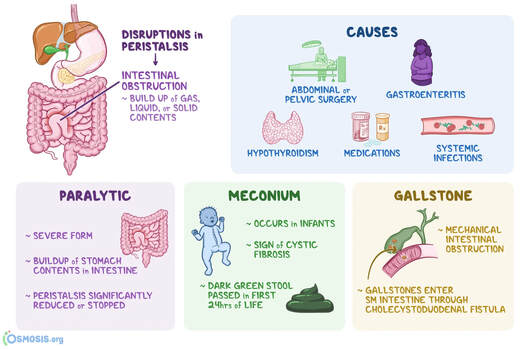
Blockage of the colon that is functional but does not have a mechanical source because of atony or abnormal peristalsis.
Etiology
Postoperative: Atonement of the bowel after intraabdominal surgery.
Metabolic conditions include liver failure, hypomagnesemia, hypokalaemia, ketoacidosis, and uraemia.
Response to an inflammatory disease, such as cholecystitis, is called infection or inflammation.
Chemical or bacterial diffuse peritonitis.
Pathology of the retroperitoneum: hemorrhage, pancreatitis.
Drugs: antipsychotics, anticholinergics, and opioids.
Scleroderma, multiple sclerosis, Parkinson's disease, and diabetes are examples of neuropathic illnesses.
Ogilvie's syndrome: Colonic pseudo-obstruction linked to polypharmacy, chronic illness, immobility, and long-term debility.
Epidemiology
depending on the cause, but a prevalent issue in people undergoing surgery. Acute colonic pseudoobstruction typically affects older people who have coexisting medical conditions.
History
Past events related to the cause, such as a recent operation. Constipation and inability to pass gas. stomach distension at first without discomfort, but later symptoms could resemble those of a real blockage.
Examination
stomach distension. There could be less or no bowel sounds. Soreness, potential problems, and/or peritonism. A rectal examination may reveal faecal impaction.
Investigations
in accordance with the aetiology and condition of the patient. Possible contents include:
FBC, U&Es, Mg2+, ESR, and CRP in blood.
Visualization: A CT scan, erect CXR and AXR, may reveal intestinal distension and faecal impaction.
>12 cm caecal diameter considerably increases the chance of perforation.A water-soluble contrast enema aids in distinguishing between an obstruction that is mechanical.
Managements
Depending on the aetiology, the following methods are frequently employed:
Nebulization by NG tube if vomiting, IV fluid replenishment, and correction of electrolyte imbalances (particularly hypokalaemia and hypomagnesaemia) are supportive measures. A flatus tube inserted could aid in decompression. Avoiding laxatives and medications that lower intestinal motility, particularly those that contain osmotic substances like lactulose.
Medical: Addressing the underlying issue, such as an infection. Prokinetic medications like metoclopramide and domperidone may be effective in treating chronic paralytic ileus in the absence of mechanical obstruction. If there is an acute colonic pseudoobstruction, IV neostigmine can be administered, but it must be well monitored due to the risk of hypotension, bradycardia, and brochospasm.
Endoscopic decompression: Has a 2% risk of perforation and can be useful in cases of colonic pseudo-obstruction.
Surgical: For severe morbidity and mortality, impending or actualized perforation. Decompression and stoma creation; in the event of complications, ileorectal anastamosis or segmental or subtotal colonic resection and exteriorization.
Complications
Bowel perforation, peritonitis, most frequently caecal (40% mortality).
Prognosis
Typically reacts to precautionary actions. Overall mortality from acute colonic pseudo-obstruction ranges from 25 to 31%.
0 Comments
