- Published on
Surgery - Intestinal Ischemia
Introduction
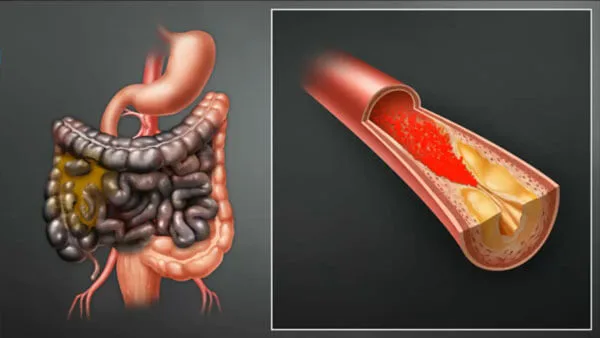
Bowel necrosis and ischemia caused by obstruction (e.g., by an embolus or thrombosis) of a mesenteric artery.
Etiology
60% in emboli, 25% in arterial thrombosis, and 15% in venous thrombosis. may result from bowel strangulation inside a hernia, volvulus, intussusception, or surgical resection.
Risk Factors
Endocarditis for emboli, atrial fibrillation, and cardiac mural thrombus. For arterial thrombosis, hypertension, diabetes mellitus, and smoking are risk factors. Venous thrombosis is linked to splenectomy, portal hypertension, septic thrombophlebitis, and heart failure.
Epidemiology
Depending on the cause. more typical among older people.
H HISTORY
severe, intense stomach pain from colickiness. possibly accompanied by rectal bleeding or vomiting.
Past medical history of persistent mesenteric artery insufficiency, including significant weight loss and pain in the abdomen after eating. past liver or heart illness.
History and Examination
diffuse soreness and distension in the abdomen. a sensitive, palpable mass if a hernia is present. There could be no bowel sounds. unequal level of cardiovascular breakdown.
Investigations
Making the diagnosis might be challenging and may depend on a laparotomy or clinical suspicion.
Blood: FBC, U&Es, LFT, clotting, crossmatch, ABG (lactic acidosis).
AXR: May reveal thumbprinting or thickening of the intestinal wall.
CT scan: The intestinal wall may contain gas.
Mesenteric arteriography: Provides localization, assessment of the degree, and trial of intervention if stable.
Management
General: IV fluid resuscitation and electrolyte imbalance correction, IV antibiotics, nil by mouth.
Surgical: Infarcted bowel resection and emergency laparotomy. An embolectomy or a saphenous vein bypass from the iliac artery to the superior mesenteric artery below the blockage can be used to restore the vascular supply to the non-necrotic colon. A transient, non-functional stoma is frequently utilized. After surgery, close observation and care are necessary, usually on an ITU or HDU. Rarely, complete parenteral nourishment has been used to support large-scale small-bowel resection, which was then followed by small-bowel transplantation.
Medical: Heparin post-operative thrombosis prevention. Warfarinization over the long term could be advised.
Complications
multi-organ failure, intestinal perforation, peritonitis, and lactic acidosis.
Prognosis
It's a grave illness with a 50–100% fatality rate.
Introduction
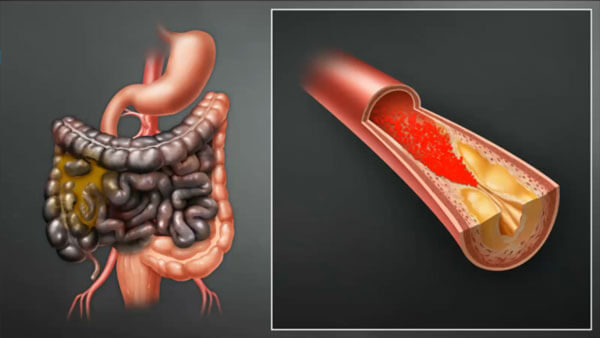
Bowel necrosis and ischemia caused by obstruction (e.g., by an embolus or thrombosis) of a mesenteric artery.
Etiology
60% in emboli, 25% in arterial thrombosis, and 15% in venous thrombosis. may result from bowel strangulation inside a hernia, volvulus, intussusception, or surgical resection.
Risk Factors
Endocarditis for emboli, atrial fibrillation, and cardiac mural thrombus. For arterial thrombosis, hypertension, diabetes mellitus, and smoking are risk factors. Venous thrombosis is linked to splenectomy, portal hypertension, septic thrombophlebitis, and heart failure.
Epidemiology
Depending on the cause. more typical among older people.
H HISTORY
severe, intense stomach pain from colickiness. possibly accompanied by rectal bleeding or vomiting.
Past medical history of persistent mesenteric artery insufficiency, including significant weight loss and pain in the abdomen after eating. past liver or heart illness.
History and Examination
diffuse soreness and distension in the abdomen. a sensitive, palpable mass if a hernia is present. There could be no bowel sounds. unequal level of cardiovascular breakdown.
Investigations
Making the diagnosis might be challenging and may depend on a laparotomy or clinical suspicion.
Blood: FBC, U&Es, LFT, clotting, crossmatch, ABG (lactic acidosis).
AXR: May reveal thumbprinting or thickening of the intestinal wall.
CT scan: The intestinal wall may contain gas.
Mesenteric arteriography: Provides localization, assessment of the degree, and trial of intervention if stable.
Management
General: IV fluid resuscitation and electrolyte imbalance correction, IV antibiotics, nil by mouth.
Surgical: Infarcted bowel resection and emergency laparotomy. An embolectomy or a saphenous vein bypass from the iliac artery to the superior mesenteric artery below the blockage can be used to restore the vascular supply to the non-necrotic colon. A transient, non-functional stoma is frequently utilized. After surgery, close observation and care are necessary, usually on an ITU or HDU. Rarely, complete parenteral nourishment has been used to support large-scale small-bowel resection, which was then followed by small-bowel transplantation.
Medical: Heparin post-operative thrombosis prevention. Warfarinization over the long term could be advised.
Complications
multi-organ failure, intestinal perforation, peritonitis, and lactic acidosis.
Prognosis
It's a grave illness with a 50–100% fatality rate.
Intestinal Ischemia
0 Comments
