- Published on
Surgery - Intracerebral Hemorrhage
Introduction
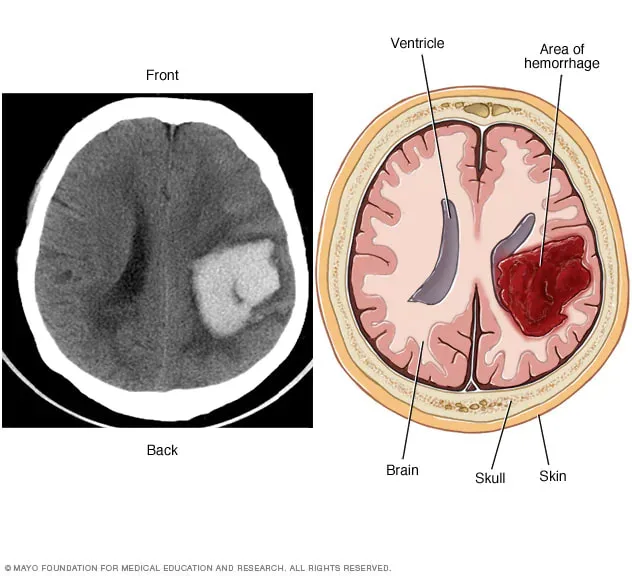
internal bleeding that results in the creation of a localized hemorrhage in the brain parenchyma.
Etiology
The two most frequent causes are trauma and hypertension. Arteriovenous malformation, intracerebral aneurysms, cavernous haemangiomas, tumors, bleeding into an area that has already been infarcted, and drug addiction (such as amphetamine and cocaine) are other reasons.
may develop either inward into the ventricular system (intraventricular hemorrhage) or outward onto the brain's surface (becoming a subarachnoid hemorrhage).
Epidemiology
15% of cases of stroke. There are 15–300/100,000 cases. maximum frequency in older age cohorts.
History
Depending on the origin of the hemorrhage, signs of sudden onset of stroke syndrome can include contralateral paralysis and speech disturbance if the dominant hemisphere is affected.
declining consciousness level.
vomiting and headaches.
Examination
Hemiparesis, sensory loss, cranial nerve abnormalities, cerebellar ataxia, and loss of higher cognitive abilities are symptoms of stroke syndrome.
Bradycardia, elevated blood pressure, and a decreased GCS are indicators of elevated ICP. A potential herniation may be indicated by uneven pupils.
Investigations
Brain CT scan: Recommended for all stroke types to differentiate between ischemic and hemorrhagic strokes.
Severity indicators include hydrocephalus, midline shift, and elevated ICP.
Brain MRI: The gradient-echo sequence is helpful in locating sites of microhaemorrhage and has a high sensitivity for haemosiderin.
If there is a suspicion that there is a vascular abnormality underlying, cerebral angiography may be necessary.
Management
Emergency: Pay close attention to ABC; GCS may need to be used for intubation and ventilation.
supportive care that includes resuscitation, coagulation and electrolyte problems repair, and other measures.
Surgery: Since the STICH-1 trial indicates no discernible advantage from early neurosurgery, craniotomy for the evacuation of hemorrhages should only be performed for big (>3 cm) cerebellar hemorrhages or those with large lobar hemorrhages, substantial mass effect, and rapidly deteriorating health.
Medical: ICP monitoring: observation (e.g., implantation of a pressure monitoring bolt) and management of elevated ICP (e.g., moving the bed upright, hyperventilation, external ventricular drain in hydrocephalus).
Blood pressure regulation: Sudden drop in blood pressure increases the chance of a watershed infarction. Though the INTERACT study has demonstrated that a goal systolic blood pressure of less than 140 mmHg is linked to a decreased risk of adverse events and a decrease in hemorrhage, standard guidelines still propose a target systolic blood pressure of less than 180 mmHg.
Supportive measures include pressure point relief, nutritional support (NG feeding), speech and language therapy, and rehabilitation.
More recent agents: Factor VII reduces hematoma expansion, however the FAST trial's outcome was unaffected.
Complications
elevated ICP, hydrocephalus, neural impairments, and herniation, particularly in cases of posterior fossa hemorrhage.
Prognosis
high mortality, with the magnitude of the hemorrhage and the GCS score upon admission serving as reliable indicators of prognosis.
Introduction
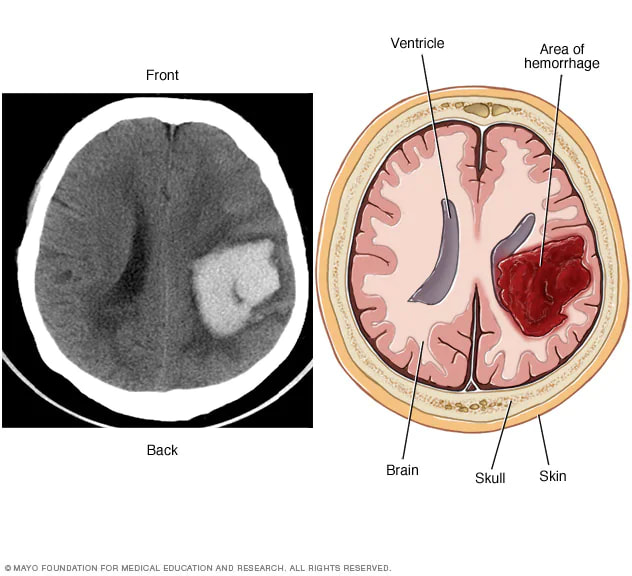
internal bleeding that results in the creation of a localized hemorrhage in the brain parenchyma.
Etiology
The two most frequent causes are trauma and hypertension. Arteriovenous malformation, intracerebral aneurysms, cavernous haemangiomas, tumors, bleeding into an area that has already been infarcted, and drug addiction (such as amphetamine and cocaine) are other reasons.
may develop either inward into the ventricular system (intraventricular hemorrhage) or outward onto the brain's surface (becoming a subarachnoid hemorrhage).
Epidemiology
15% of cases of stroke. There are 15–300/100,000 cases. maximum frequency in older age cohorts.
History
Depending on the origin of the hemorrhage, signs of sudden onset of stroke syndrome can include contralateral paralysis and speech disturbance if the dominant hemisphere is affected.
declining consciousness level.
vomiting and headaches.
Examination
Hemiparesis, sensory loss, cranial nerve abnormalities, cerebellar ataxia, and loss of higher cognitive abilities are symptoms of stroke syndrome.
Bradycardia, elevated blood pressure, and a decreased GCS are indicators of elevated ICP. A potential herniation may be indicated by uneven pupils.
Investigations
Brain CT scan: Recommended for all stroke types to differentiate between ischemic and hemorrhagic strokes.
Severity indicators include hydrocephalus, midline shift, and elevated ICP.
Brain MRI: The gradient-echo sequence is helpful in locating sites of microhaemorrhage and has a high sensitivity for haemosiderin.
If there is a suspicion that there is a vascular abnormality underlying, cerebral angiography may be necessary.
Management
Emergency: Pay close attention to ABC; GCS may need to be used for intubation and ventilation.
supportive care that includes resuscitation, coagulation and electrolyte problems repair, and other measures.
Surgery: Since the STICH-1 trial indicates no discernible advantage from early neurosurgery, craniotomy for the evacuation of hemorrhages should only be performed for big (>3 cm) cerebellar hemorrhages or those with large lobar hemorrhages, substantial mass effect, and rapidly deteriorating health.
Medical: ICP monitoring: observation (e.g., implantation of a pressure monitoring bolt) and management of elevated ICP (e.g., moving the bed upright, hyperventilation, external ventricular drain in hydrocephalus).
Blood pressure regulation: Sudden drop in blood pressure increases the chance of a watershed infarction. Though the INTERACT study has demonstrated that a goal systolic blood pressure of less than 140 mmHg is linked to a decreased risk of adverse events and a decrease in hemorrhage, standard guidelines still propose a target systolic blood pressure of less than 180 mmHg.
Supportive measures include pressure point relief, nutritional support (NG feeding), speech and language therapy, and rehabilitation.
More recent agents: Factor VII reduces hematoma expansion, however the FAST trial's outcome was unaffected.
Complications
elevated ICP, hydrocephalus, neural impairments, and herniation, particularly in cases of posterior fossa hemorrhage.
Prognosis
high mortality, with the magnitude of the hemorrhage and the GCS score upon admission serving as reliable indicators of prognosis.
0 Comments
