- Published on
Surgery - Intussusception
Introduction
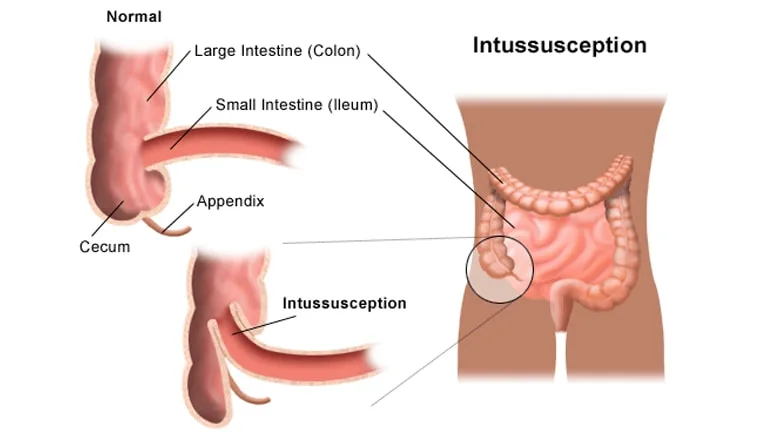
the process of an intestine segment, the intussusceptum, invaginating into the adjacent intestinal lumen, the intussuscipiens, with the potential to cause blockage or vascular compromise of the colon.
Etiology
<three years: Up to 90% of cases are idiopathic and are linked to lymphoid hyperplasia in Peyer's patches, Meckel's diverticulum, polyps, and hemorrhages.
Children: Henoch-Schönlein purpura, blood dyscrasias (caused by submucosal hemoglobinas), recent upper respiratory tract infections.
Child/Adult: About one-third of small-bowel cases and two-thirds of large-bowel cases involve a mass in the bowel wall or lumen, such as a polyp, tumor, or Meckel's diverticulum, that is caused by malignancy.
Epidemiology
The frequency is 1-3/1000. mostly affects children between the ages of three and nine months. uncommon among grownups.
H HISTORY
Children may experience sporadic episodes of intense stomach discomfort, frequently accompanied by limb cramping. It is reported that PR can pass bloody mucus that looks like "red currant jelly."
Later stages may have vomiting and distension, similar to intestinal obstruction. Adults may experience vague symptoms.
Examination
Traditionally, the right hypochondrium had a "sausage-shaped" bulk.
Pale, hypotensive, and tachycardic are signs of shock.
Abdominal distension and tinkling bowel noises are indicators of blockage.
Absence of bowel sounds, rebound, and abdominal guarding are symptoms of peritonism.
Pathogenesis
The gut exhibits aberrant telescoping and peristalsis due to a pathological "lead point." The most frequent location is the ileocolic junction, however ileo-ileal and colo-colic are also possible. If left untreated, bowel wall venous congestion and oedema can lead to infarction and perforation.
Investigational studies
AXR: May reveal signs of blockage or a lack of air in the right side of the colon.
Ultrasound: The intruded section manifests as a lump shaped like a target.
The traditional method of demonstrating intussusception is with contrast/air enema, where the contrast at the location resembles a "coiled spring." Therapy may result from this (see Management).
Blood: lactic acidosis-related ABG, G&S, U&Es, and FBC.
Management
Supportive measures include NG tube insertion if vomiting, analgesics, antibiotic cover, and IV fluid resuscitation.
Therapeutic enema: Barium, air, or saline can be used to reduce the invaginating segment back. Not recommended in cases of suspected tumor, peritonitis, or perforation.
Surgery: Done if an enema is unable to relieve the condition or if peritonitis is showing symptoms.
To lessen intussusception, the impacted bowel is gently moved. Resection of the affected segment is required if the implicated bowel is non-viable, cannot be shrunk, or Meckel's diverticulum is discovered. able could be carried out laparoscopically
Complications
can result in perforation, blockage, hemorrhage, and ischaemia.
Prognosis
In as many as 10% of pediatric instances, spontaneous decrease can happen. The rate of recurrence is 5–10%.
Good with quick care; if left untreated, could be lethal.
Introduction
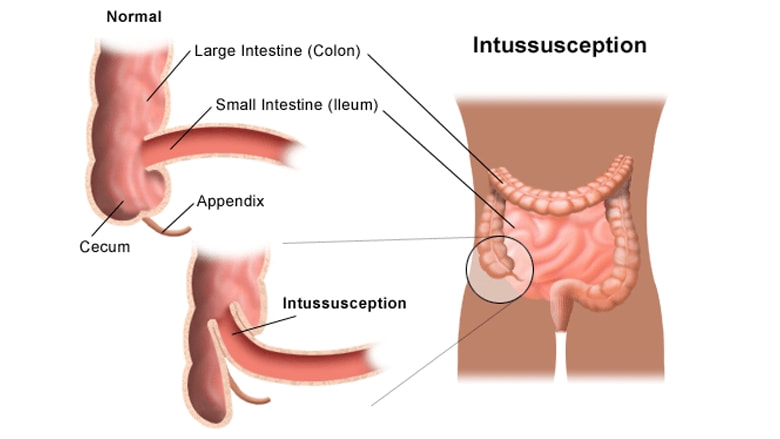
the process of an intestine segment, the intussusceptum, invaginating into the adjacent intestinal lumen, the intussuscipiens, with the potential to cause blockage or vascular compromise of the colon.
Etiology
<three years: Up to 90% of cases are idiopathic and are linked to lymphoid hyperplasia in Peyer's patches, Meckel's diverticulum, polyps, and hemorrhages.
Children: Henoch-Schönlein purpura, blood dyscrasias (caused by submucosal hemoglobinas), recent upper respiratory tract infections.
Child/Adult: About one-third of small-bowel cases and two-thirds of large-bowel cases involve a mass in the bowel wall or lumen, such as a polyp, tumor, or Meckel's diverticulum, that is caused by malignancy.
Epidemiology
The frequency is 1-3/1000. mostly affects children between the ages of three and nine months. uncommon among grownups.
H HISTORY
Children may experience sporadic episodes of intense stomach discomfort, frequently accompanied by limb cramping. It is reported that PR can pass bloody mucus that looks like "red currant jelly."
Later stages may have vomiting and distension, similar to intestinal obstruction. Adults may experience vague symptoms.
Examination
Traditionally, the right hypochondrium had a "sausage-shaped" bulk.
Pale, hypotensive, and tachycardic are signs of shock.
Abdominal distension and tinkling bowel noises are indicators of blockage.
Absence of bowel sounds, rebound, and abdominal guarding are symptoms of peritonism.
Pathogenesis
The gut exhibits aberrant telescoping and peristalsis due to a pathological "lead point." The most frequent location is the ileocolic junction, however ileo-ileal and colo-colic are also possible. If left untreated, bowel wall venous congestion and oedema can lead to infarction and perforation.
Investigational studies
AXR: May reveal signs of blockage or a lack of air in the right side of the colon.
Ultrasound: The intruded section manifests as a lump shaped like a target.
The traditional method of demonstrating intussusception is with contrast/air enema, where the contrast at the location resembles a "coiled spring." Therapy may result from this (see Management).
Blood: lactic acidosis-related ABG, G&S, U&Es, and FBC.
Management
Supportive measures include NG tube insertion if vomiting, analgesics, antibiotic cover, and IV fluid resuscitation.
Therapeutic enema: Barium, air, or saline can be used to reduce the invaginating segment back. Not recommended in cases of suspected tumor, peritonitis, or perforation.
Surgery: Done if an enema is unable to relieve the condition or if peritonitis is showing symptoms.
To lessen intussusception, the impacted bowel is gently moved. Resection of the affected segment is required if the implicated bowel is non-viable, cannot be shrunk, or Meckel's diverticulum is discovered. able could be carried out laparoscopically
Complications
can result in perforation, blockage, hemorrhage, and ischaemia.
Prognosis
In as many as 10% of pediatric instances, spontaneous decrease can happen. The rate of recurrence is 5–10%.
Good with quick care; if left untreated, could be lethal.
0 Comments
