- Published on
Surgery -Laparoscopic Abdominal Surgery
Indications
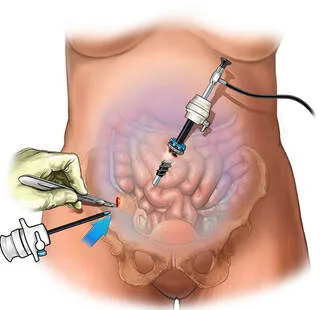
minimal access surgery of the abdomen or pelvis, in which a laparoscopic camera (either at a 0°, 30°, or 45° angle) is inserted through a port into the peritoneal cavity for inspection and to direct the manipulation of additional instruments inserted through other ports after a CO2 pneumoperitoneum has been created.
Diagnostic: Used for directed biopsy or emergency assessment of abdominal trauma, as well as for the study of abdominal or pelvic pain, focused liver illness, abdominal masses, and the staging of malignant disease.
Therapeutic: A lot of procedures involving the abdomen can now be completed with minimally invasive techniques. Laparoscopic cholecystectomy, appendixectomy, fundoplication, colectomies, hernia repairs, nephrectomy, prostatectomy, and bariatric operations are among the frequently performed procedures. Other operations, such as laparoscopic-assisted hysterectomy, can benefit from laparoscopy assistance.
Relative contraindications include respiratory insufficiency, the existence of dilated colon, and untreated coagulopathy. Conversion to open surgery may be more likely if prior open surgery was performed ("likelihood of adhesions").
Anatomy
In otherwise healthy patients, the physiological effects of a pneumoperitoneum are typically well tolerated; however, patients with heart disease may find them more difficult to bear.
Cardiovascular: decreased cardiac output; elevated pulmonary and systemic vascular resistance; elevated cardiac preload; decreased renal, hepatic, and splanchnic flow.
Renin and aldosterone, sympathomimetic reaction, and renal vasoconstriction are examples of metabolic and autonomic processes.
Investigational studies
Blood: coagulation and FBC.
as suitable for the planned process.
Actions
carried out while under general anesthesia.
Preparation: Depending on the planned procedure, a nasogastric tube or urinary catheterization can be used to decompress the bladder and stomach, respectively. The abdominal cavity is prepared and draped.
Pneumoperitoneum: There are three ways to gain access to the peritoneal cavity:
Open (Hassan): The fascia is visible after the initial incision. This is separated, and the Hassan trocar can be fastened using fascial sutures. Using two tissue forceps, the peritoneum is gripped, then the peritoneal cavity is forcefully opened, the Hassan trocar is put into it under direct vision, and insufflation is initiated.
Closed Veress needle: The peritoneal cavity is punctured using a Veress needle. There are two areas of resistance in the midline—the fascia and the peritoneum—and three points of resistance farther laterally—the anterior and posterior sheaths and the peritoneum. The free passage of salt aids in verifying accurate positioning. Low CO2 insufflation pressure is ideal; if it's high, move the needle. After the establishment of the pneumoperitoneum, the trocar is placed and the needle is removed. Because this is a blind treatment, there is a greater risk of injury to blood vessels or the bowel.
Optical trocar: Using a transparent, bladeless trocar and a 0 degree laparoscope, the layers of the abdominal wall can be seen while the trocar is being advanced through the wall by applying direct pressure and twisting. beneficial for those who are fat.
Laparoscope insertion: The laparoscope is used to view the peritoneal cavity and safely direct the insertion of additional ports. It is inserted after the white balance has been adjusted to account for the yellow light of the halogen bulb.
Closure: To ensure there is no bleeding, the instruments and ports are removed under direct eyesight, in accordance with the intended process. Pneumoperitoneum deflation and proper wound closure are carried out. Fascial closure is often not necessary for 5mm ports, but depending on their location, bigger ports (10–12 mm) frequently require it to prevent herniation.
Complications
Immediate : Extraperitoneal insufflation, damage to the viscera or vessels (vascular injuries reported to occur 0.04–0.5%, visceral injuries 0.06–0.12%), and open Hassan technique against Veress needle or optical trocar had fewer incidences. diaphragmatic splinting brought on by a high inhalation pressure. Pneumothorax and gas embolism are uncommon.
Early signs and symptoms include shoulder tip pain, wound infection, and the aftereffects of an undiagnosed visceral injury (such as peritonitis after a bowel injury or bile duct damage).
Late : Incisional hernia
Indications
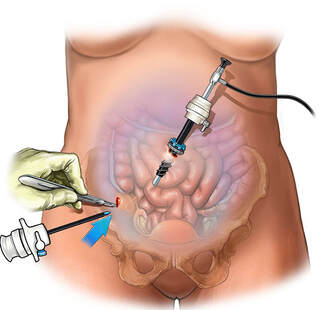
minimal access surgery of the abdomen or pelvis, in which a laparoscopic camera (either at a 0°, 30°, or 45° angle) is inserted through a port into the peritoneal cavity for inspection and to direct the manipulation of additional instruments inserted through other ports after a CO2 pneumoperitoneum has been created.
Diagnostic: Used for directed biopsy or emergency assessment of abdominal trauma, as well as for the study of abdominal or pelvic pain, focused liver illness, abdominal masses, and the staging of malignant disease.
Therapeutic: A lot of procedures involving the abdomen can now be completed with minimally invasive techniques. Laparoscopic cholecystectomy, appendixectomy, fundoplication, colectomies, hernia repairs, nephrectomy, prostatectomy, and bariatric operations are among the frequently performed procedures. Other operations, such as laparoscopic-assisted hysterectomy, can benefit from laparoscopy assistance.
Relative contraindications include respiratory insufficiency, the existence of dilated colon, and untreated coagulopathy. Conversion to open surgery may be more likely if prior open surgery was performed ("likelihood of adhesions").
Anatomy
In otherwise healthy patients, the physiological effects of a pneumoperitoneum are typically well tolerated; however, patients with heart disease may find them more difficult to bear.
Cardiovascular: decreased cardiac output; elevated pulmonary and systemic vascular resistance; elevated cardiac preload; decreased renal, hepatic, and splanchnic flow.
Renin and aldosterone, sympathomimetic reaction, and renal vasoconstriction are examples of metabolic and autonomic processes.
Investigational studies
Blood: coagulation and FBC.
as suitable for the planned process.
Actions
carried out while under general anesthesia.
Preparation: Depending on the planned procedure, a nasogastric tube or urinary catheterization can be used to decompress the bladder and stomach, respectively. The abdominal cavity is prepared and draped.
Pneumoperitoneum: There are three ways to gain access to the peritoneal cavity:
Open (Hassan): The fascia is visible after the initial incision. This is separated, and the Hassan trocar can be fastened using fascial sutures. Using two tissue forceps, the peritoneum is gripped, then the peritoneal cavity is forcefully opened, the Hassan trocar is put into it under direct vision, and insufflation is initiated.
Closed Veress needle: The peritoneal cavity is punctured using a Veress needle. There are two areas of resistance in the midline—the fascia and the peritoneum—and three points of resistance farther laterally—the anterior and posterior sheaths and the peritoneum. The free passage of salt aids in verifying accurate positioning. Low CO2 insufflation pressure is ideal; if it's high, move the needle. After the establishment of the pneumoperitoneum, the trocar is placed and the needle is removed. Because this is a blind treatment, there is a greater risk of injury to blood vessels or the bowel.
Optical trocar: Using a transparent, bladeless trocar and a 0 degree laparoscope, the layers of the abdominal wall can be seen while the trocar is being advanced through the wall by applying direct pressure and twisting. beneficial for those who are fat.
Laparoscope insertion: The laparoscope is used to view the peritoneal cavity and safely direct the insertion of additional ports. It is inserted after the white balance has been adjusted to account for the yellow light of the halogen bulb.
Closure: To ensure there is no bleeding, the instruments and ports are removed under direct eyesight, in accordance with the intended process. Pneumoperitoneum deflation and proper wound closure are carried out. Fascial closure is often not necessary for 5mm ports, but depending on their location, bigger ports (10–12 mm) frequently require it to prevent herniation.
Complications
Immediate : Extraperitoneal insufflation, damage to the viscera or vessels (vascular injuries reported to occur 0.04–0.5%, visceral injuries 0.06–0.12%), and open Hassan technique against Veress needle or optical trocar had fewer incidences. diaphragmatic splinting brought on by a high inhalation pressure. Pneumothorax and gas embolism are uncommon.
Early signs and symptoms include shoulder tip pain, wound infection, and the aftereffects of an undiagnosed visceral injury (such as peritonitis after a bowel injury or bile duct damage).
Late : Incisional hernia
0 Comments
