- Published on
Surgery - Liver Transplantation
Indications
In the UK, between 600 and 700 liver transplants are performed each year in accredited facilities offering interdisciplinary care.
Elective: For end-stage liver disease, such as cirrhosis, which can lead to complications such diuretic-resistant ascites, recurrent spontaneous bacterial peritonitis, hepatorenal syndrome, and recurrent varicella hemorrhage. Biliary atresia is the most typical sign in children. The Model for End-Stage Liver Disease (MELD) scoring system, which is based on bilirubin, creatinine, and INR, or the Pediatric End-Stage Liver Disease scoring system, which is based on albumin, bilirubin, INR, growth failure, and age at listing, determine the severity of the condition before allocating organs. When diagnosing hepatocellular cancer, the "Milan criteria" are applied: one tumor <5 cm or three lesions <3 cm.
Emergency: Acute liver failure, with paracetamol overdose, viral hepatitis, and peculiar medication reactions being the most frequent causes.
Anatomy
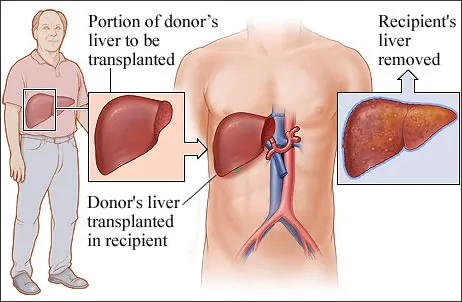
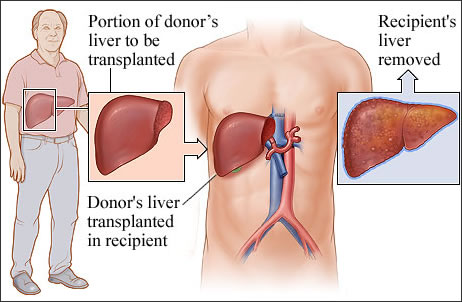
Orthoptic transplantation, often known as liver transplantation, is removing the damaged liver and replacing it with a graft in the natural hepatic bed. Although the recipient's vena cava is preserved using a different method called the "piggyback" approach, the retrohepatic part of the inferior vena cava is typically removed along with the recipient's liver. Splitting adult donor organs and segmental liver transplantation (e.g., segments 2 and 3) are done on minors.
Investigations
Pre-op: Before being put on the waiting list, patients have a thorough and in-depth examination. This comprises an ECG and echocardiography database, liver biopsy, blood grouping, tissue typing, ABG, imaging (USS, CT scans of the abdomen, head, and chest), and other evaluations, such as reviews of dentistry and psychiatry. Following organ allocation, the patient undergoes sepsis screening using ascitic tap, CXR, MSU, and blood cultures.
After surgery: Initial care involves intensive observation, antibiotics, and immunosuppression in an intensive care unit.
Procedure
The majority of donated organs come from heart-pounding individuals who have experienced brainstem death.
There are currently no objective markers of liver quality or status; instead, surgeons' subjective assessments of the liver's texture and fat content are used. The use of living relatives as donors is growing; one example is the donor's right hemihepatectomy. Blood type and weight are used to match donors and recipients.
Organ retrieval: Takes place when retrieving many organs. The hepatic artery, portal vein, bile duct, and supra- and infrahepatic IVC are dissected once the liver is mobilized. The University of Wisconsin solution or another cold preservation solution is quickly infused into the liver by cannulas placed into the portal vein and aortic arteries. The biliary system is flushed with a preservative solution after the liver and its related arteries are removed. The maximum storage duration is 15–18 hours; the shorter the preservation period, the better the outcomes.
Recipient operation: Due to related portal hypertension and coagulation problems, this procedure is frequently technically challenging. Blood product transfusions need close, intrusive monitoring; however, this can be minimized by using a cell saver, which gathers, cleans, and reuses red blood cells.
Access is gained through a "Mercedes-Benz incision." The bile duct and vasculature are severed, and the liver is mobilized.
Hepatectomy: Recipient hepatectomy entails clamping the IVC. Veno-venous bypass is employed to divert flow from the IVC, returning via an axillary or jugular vein, in patients who are unlikely to tolerate the ensuing drop in cardiac output.
Graft anastomosis: The donor liver is then anastomosed end-to-end or over a T-tube into the bile duct via the portal vein, hepatic artery, suprahepatic IVC, and infrahepatic IVC. It may be necessary to execute a Roux-en-Y choledochoenterostomy if the recipient bile duct is diseased.
Immunosuppression: Usually involves the use of an antimetabolite, such as mycophenolate mofetil, together with a calcineurin inhibitor, such as tacrolimus along with corticosteroids. LFT monitoring and transplanted liver biopsy (often through transjugular route) are used to screen for rejection.
Complications
<7% of first grafts fail or fail to function, which is a significant problem that necessitates retransplantation.
Vascular: Portal vein thrombosis, hepatic artery thrombosis, and hemorrhage are rare examples.
Biliary: Anastomotic stenosis followed by bile leakage.
Opportunistic infections: CMV and fungal infections are examples of infections.
Rejecting: Acute: Often brought on by T cells fighting the graft, this condition is managed with IV steroid shots or antibody therapy (antithymocyte globulin).
Chronic (less than 5%): Develops after the first year and is linked to progressively worsening jaundice.
Histology reveals tiny artery occlusions and "vanishing bile ducts," which typically necessitate retransplantation.
Recurrent liver disease: Reinfection is typical in cases of hepatitis B or C (if the infection was first present), with the latter potentially developing aggressively and quickly.
Hepatitis B can be treated with immunization and HB-Ig. In addition to autoimmune hepatitis, PBC, PSC, and recidivism in cases of alcoholic liver disease, there are other diseases that can recur.
Immunosuppressive complications include drug side effects, infections, diabetes, and post-transplant tumors, such as lymphomas and skin cancers.
Prognosis
Overall, survival rates are high, standing at 85% after a year and 70% after ten.
Indications
In the UK, between 600 and 700 liver transplants are performed each year in accredited facilities offering interdisciplinary care.
Elective: For end-stage liver disease, such as cirrhosis, which can lead to complications such diuretic-resistant ascites, recurrent spontaneous bacterial peritonitis, hepatorenal syndrome, and recurrent varicella hemorrhage. Biliary atresia is the most typical sign in children. The Model for End-Stage Liver Disease (MELD) scoring system, which is based on bilirubin, creatinine, and INR, or the Pediatric End-Stage Liver Disease scoring system, which is based on albumin, bilirubin, INR, growth failure, and age at listing, determine the severity of the condition before allocating organs. When diagnosing hepatocellular cancer, the "Milan criteria" are applied: one tumor <5 cm or three lesions <3 cm.
Emergency: Acute liver failure, with paracetamol overdose, viral hepatitis, and peculiar medication reactions being the most frequent causes.
Anatomy
Orthoptic transplantation, often known as liver transplantation, is removing the damaged liver and replacing it with a graft in the natural hepatic bed. Although the recipient's vena cava is preserved using a different method called the "piggyback" approach, the retrohepatic part of the inferior vena cava is typically removed along with the recipient's liver. Splitting adult donor organs and segmental liver transplantation (e.g., segments 2 and 3) are done on minors.
Investigations
Pre-op: Before being put on the waiting list, patients have a thorough and in-depth examination. This comprises an ECG and echocardiography database, liver biopsy, blood grouping, tissue typing, ABG, imaging (USS, CT scans of the abdomen, head, and chest), and other evaluations, such as reviews of dentistry and psychiatry. Following organ allocation, the patient undergoes sepsis screening using ascitic tap, CXR, MSU, and blood cultures.
After surgery: Initial care involves intensive observation, antibiotics, and immunosuppression in an intensive care unit.
Procedure
The majority of donated organs come from heart-pounding individuals who have experienced brainstem death.
There are currently no objective markers of liver quality or status; instead, surgeons' subjective assessments of the liver's texture and fat content are used. The use of living relatives as donors is growing; one example is the donor's right hemihepatectomy. Blood type and weight are used to match donors and recipients.
Organ retrieval: Takes place when retrieving many organs. The hepatic artery, portal vein, bile duct, and supra- and infrahepatic IVC are dissected once the liver is mobilized. The University of Wisconsin solution or another cold preservation solution is quickly infused into the liver by cannulas placed into the portal vein and aortic arteries. The biliary system is flushed with a preservative solution after the liver and its related arteries are removed. The maximum storage duration is 15–18 hours; the shorter the preservation period, the better the outcomes.
Recipient operation: Due to related portal hypertension and coagulation problems, this procedure is frequently technically challenging. Blood product transfusions need close, intrusive monitoring; however, this can be minimized by using a cell saver, which gathers, cleans, and reuses red blood cells.
Access is gained through a "Mercedes-Benz incision." The bile duct and vasculature are severed, and the liver is mobilized.
Hepatectomy: Recipient hepatectomy entails clamping the IVC. Veno-venous bypass is employed to divert flow from the IVC, returning via an axillary or jugular vein, in patients who are unlikely to tolerate the ensuing drop in cardiac output.
Graft anastomosis: The donor liver is then anastomosed end-to-end or over a T-tube into the bile duct via the portal vein, hepatic artery, suprahepatic IVC, and infrahepatic IVC. It may be necessary to execute a Roux-en-Y choledochoenterostomy if the recipient bile duct is diseased.
Immunosuppression: Usually involves the use of an antimetabolite, such as mycophenolate mofetil, together with a calcineurin inhibitor, such as tacrolimus along with corticosteroids. LFT monitoring and transplanted liver biopsy (often through transjugular route) are used to screen for rejection.
Complications
<7% of first grafts fail or fail to function, which is a significant problem that necessitates retransplantation.
Vascular: Portal vein thrombosis, hepatic artery thrombosis, and hemorrhage are rare examples.
Biliary: Anastomotic stenosis followed by bile leakage.
Opportunistic infections: CMV and fungal infections are examples of infections.
Rejecting: Acute: Often brought on by T cells fighting the graft, this condition is managed with IV steroid shots or antibody therapy (antithymocyte globulin).
Chronic (less than 5%): Develops after the first year and is linked to progressively worsening jaundice.
Histology reveals tiny artery occlusions and "vanishing bile ducts," which typically necessitate retransplantation.
Recurrent liver disease: Reinfection is typical in cases of hepatitis B or C (if the infection was first present), with the latter potentially developing aggressively and quickly.
Hepatitis B can be treated with immunization and HB-Ig. In addition to autoimmune hepatitis, PBC, PSC, and recidivism in cases of alcoholic liver disease, there are other diseases that can recur.
Immunosuppressive complications include drug side effects, infections, diabetes, and post-transplant tumors, such as lymphomas and skin cancers.
Prognosis
Overall, survival rates are high, standing at 85% after a year and 70% after ten.
0 Comments
