- Published on
Surgery - Neck of Femur Fracture
Introduction
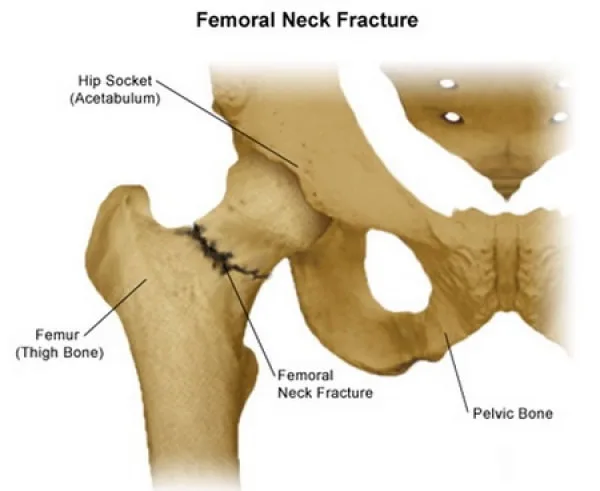
disruption in the femur's cortical bone continuity at or above the lesser trochanter.
There are two categories into which fractures fall:
Intracapsular: Including subcapital, transcervical, and basicervical; occurs close to the point where the hip joint capsule joins the femur.
Extracapsular: Subtrochanteric or trochanteric
Etiology
osteoporosis and a higher frequency of falls among the elderly; additional risk factors include smoking at the moment, having a BMI below 18.5, having had a mild trauma fracture after age 50, having a mother who has had a hip fracture, hyperparathyroidism, and Paget's disease.
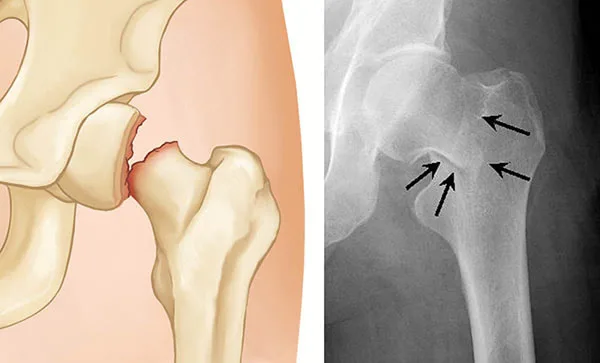
anatomy Since the retinacular arteries that travel back along the capsule are the primary source of blood supply to the femoral head, intracapsular fractures have the potential to disrupt this supply and cause avascular necrosis.
Epidemiology
Frequent in the elderly; lifetime risk for women is 18%, for men it is 6%. 12/100 (over 85 years old), 3/100 (65–74 years old).
History
Hip pain and movement restriction may arise from a slight fall in the past.
Examination
There is hip pain and the affected leg is shortened, adducted, and externally rotated.
Investigations
Blood: coagulation, G&S, U&Es, and FBC.
Imaging: Lateral images of the hip and plain AP radiographs. If the diagnosis is unclear, an MRI, a bone scan, or further plain radiographs should be taken 24 to 48 hours later. CXR in case elderly patients need surgery.
Management
Prevention: Risk evaluation and fall-risk reduction measures.
Medical: For primary or secondary prophylaxis, calcium, vitamin D, HRT, selective oestrogen receptor modulators, bisphosphonates, calciumitonin, fluoride, and thiazides have been utilized.
Prompt: Analgesia, resuscitation, electrolyte and fluid imbalance correction, pressure area care. It is recommended that patients undergo surgery within a day to minimize the possibility of thrombotic problems and pressure damage.
Undisplaced intracapsular fractures: Hemiarthroplasty may be taken into consideration in the extremely old; internal fixation permits early mobilization and lowers the chance of fractures becoming displaced.
Displaced intracapsular fractures: Hemiarthroplasty or total hip replacement (may be acceptable in patients with pre-existing joint illness, good activity levels, and a fair life expectancy), open reduction and internal fixation (for younger, more active patients).
Unless there is a medical reason not to, extracapsular fractures should be surgically treated with reduction and internal fixation using either intramedullary (such as gamma nail implants) or extramedullary (such as sliding screws and plates).
Antibiotic prophylaxis during induction and DVT prevention have to be administered to all patients.
Complications
Early symptoms include pain, immobility, infections, pressure sores (20%), pulmonary problems (ARDS, fat embolism, pneumonia), DVT (asymptomatic up to 45%, symptomatic up to 11%), and PE (3–13%).
Implant failure, non-union, and avascular necrosis of the femur head are late symptoms.
Prognosis
After a hip fracture, the elderly have a high death rate (30% at one year), with 25% needing more extensive long-term care.
Introduction
disruption in the femur's cortical bone continuity at or above the lesser trochanter.
There are two categories into which fractures fall:
Intracapsular: Including subcapital, transcervical, and basicervical; occurs close to the point where the hip joint capsule joins the femur.
Extracapsular: Subtrochanteric or trochanteric
Etiology
osteoporosis and a higher frequency of falls among the elderly; additional risk factors include smoking at the moment, having a BMI below 18.5, having had a mild trauma fracture after age 50, having a mother who has had a hip fracture, hyperparathyroidism, and Paget's disease.
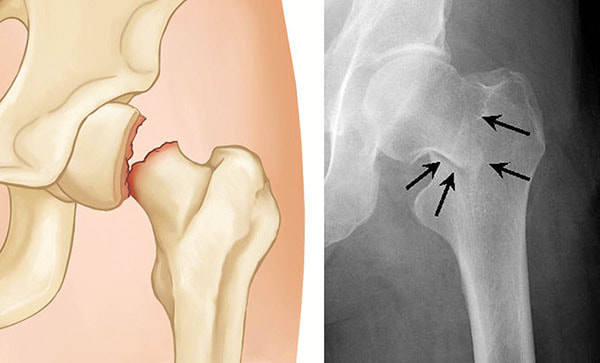
anatomy Since the retinacular arteries that travel back along the capsule are the primary source of blood supply to the femoral head, intracapsular fractures have the potential to disrupt this supply and cause avascular necrosis.
Epidemiology
Frequent in the elderly; lifetime risk for women is 18%, for men it is 6%. 12/100 (over 85 years old), 3/100 (65–74 years old).
History
Hip pain and movement restriction may arise from a slight fall in the past.
Examination
There is hip pain and the affected leg is shortened, adducted, and externally rotated.
Investigations
Blood: coagulation, G&S, U&Es, and FBC.
Imaging: Lateral images of the hip and plain AP radiographs. If the diagnosis is unclear, an MRI, a bone scan, or further plain radiographs should be taken 24 to 48 hours later. CXR in case elderly patients need surgery.
Management
Prevention: Risk evaluation and fall-risk reduction measures.
Medical: For primary or secondary prophylaxis, calcium, vitamin D, HRT, selective oestrogen receptor modulators, bisphosphonates, calciumitonin, fluoride, and thiazides have been utilized.
Prompt: Analgesia, resuscitation, electrolyte and fluid imbalance correction, pressure area care. It is recommended that patients undergo surgery within a day to minimize the possibility of thrombotic problems and pressure damage.
Undisplaced intracapsular fractures: Hemiarthroplasty may be taken into consideration in the extremely old; internal fixation permits early mobilization and lowers the chance of fractures becoming displaced.
Displaced intracapsular fractures: Hemiarthroplasty or total hip replacement (may be acceptable in patients with pre-existing joint illness, good activity levels, and a fair life expectancy), open reduction and internal fixation (for younger, more active patients).
Unless there is a medical reason not to, extracapsular fractures should be surgically treated with reduction and internal fixation using either intramedullary (such as gamma nail implants) or extramedullary (such as sliding screws and plates).
Antibiotic prophylaxis during induction and DVT prevention have to be administered to all patients.
Complications
Early symptoms include pain, immobility, infections, pressure sores (20%), pulmonary problems (ARDS, fat embolism, pneumonia), DVT (asymptomatic up to 45%, symptomatic up to 11%), and PE (3–13%).
Implant failure, non-union, and avascular necrosis of the femur head are late symptoms.
Prognosis
After a hip fracture, the elderly have a high death rate (30% at one year), with 25% needing more extensive long-term care.

0 Comments
