- Published on
Surgery - Pancreatoduodenectomy, or Whipple's Procedure
Indications
tumors of the ampulla, distal common bile duct, duodenum, or head of the pancreas (usually, less than 20% of patients have curable disease).
Anatomy
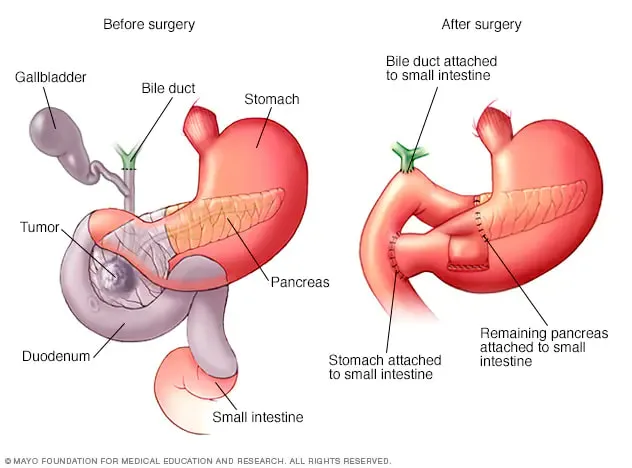
In the transpyloric plane, the pancreas is a retroperitoneal structure. The head, neck, body, and tail make up the four sections. The duodenum's curvature contains the head.During a Whipple's procedure, the distal stomach, duodenum, head of the pancreas, distal common bile duct, and gallbladde are removed all at once (with the exception of pylorus-preserving pancreatectomy).
By creating a pancreaticojejunostomy, choledochojejunostomy, and gastrojejunostomy, one can maintain intestinal continuity. In recent times, there has been evidence that pylorus-preserving pancreaticoduodenectomy enhances gastrointestinal function, as demonstrated by reduced ulceration, dumping syndrome, and enhanced weight gain.
Vascular: The splenic and pancreaticoduodenal arteries provide blood to the pancreas.
The pancreaticoduodenal and splenic veins lead to the portal vein via venous drainage.
Investigations
Endoscopy/ERCP: histology and diagnosis.
Imaging: FDG-PET scans, endoscopic ultrasonography, angiography, CT, and MRCP for staging, diagnosis, and resectability evaluation.
FBC, U&E, LFT, CA19-9, and CEA in blood.
Pre-operative care may involve biliary decompression or stenting, blood and crossmatch, and multidisciplinary discussion. Use broad-spectrum antibiotics to cover.
Following surgery, post-operative treatment should include ICU/HDU supervision, insulin to regulate blood sugar, H2 receptor antagonists or proton pump inhibitors, octreotide and thromboprophylaxis, and, in the long run, pancreatic enzyme supplements. Perhaps adjuvant chemoradiotherapy is necessary.
Procedure
Supine position is used.
Rooftop, vertical midline, or transverse incisions are all possible.
Examination: Resectability of lesion and contents of abdomen assessed. Palliation via bypass, such as gastrojejunostomy and choledocho- or cholecystojejunostomy, if it is incurable.
Mobilization: In a pylorus-preserving surgery, the duodenum is mobilized (Kocherization) and the distal stomach is divided or the duodenum is divided 2 cm distal to the pylorus. Along with the gallbladder, common bile duct, and proximal pancreas, the duodenum is removed along with lymph nodes. To guarantee distinct margins during pancreatic resection, utilize frozen section. One can conduct an end-to-end or side-to-side pancreaticojejunostomy. An end-to-side pylorus-jejunotomy, end-to-side gastrojejunostomy, and end-to-side hepaticojejunostomy are made further downstream. You can create a feeding jejunostomy to provide nutritional support.
Conclusion: prudent hemostasis. The positioning of drains. Mass closure. Skin can be sealed using clips or subcuticular sutures.
Complications
The rate of morbidity is 40%. bleeding, dumping, reflux, anastomotic leak, biliary leak, ileus, hyperglycemia, sepsis from an abdomen or wound, delayed gastric emptying, pancreatitis, pancreatic fistula, and pancreatic insufficiency.
Prognosis
This is a significant surgical procedure that need to be carried out in specialized hospitals with current death rates around 5%. 30% of 5-year survival rates for resectable tumors.
Indications
tumors of the ampulla, distal common bile duct, duodenum, or head of the pancreas (usually, less than 20% of patients have curable disease).
Anatomy
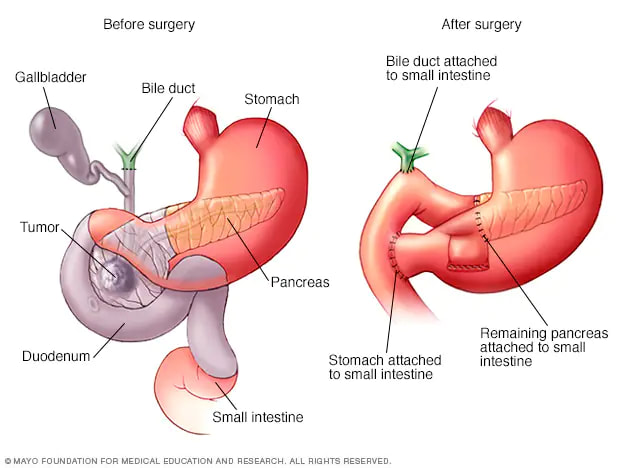
In the transpyloric plane, the pancreas is a retroperitoneal structure. The head, neck, body, and tail make up the four sections. The duodenum's curvature contains the head.During a Whipple's procedure, the distal stomach, duodenum, head of the pancreas, distal common bile duct, and gallbladde are removed all at once (with the exception of pylorus-preserving pancreatectomy).
By creating a pancreaticojejunostomy, choledochojejunostomy, and gastrojejunostomy, one can maintain intestinal continuity. In recent times, there has been evidence that pylorus-preserving pancreaticoduodenectomy enhances gastrointestinal function, as demonstrated by reduced ulceration, dumping syndrome, and enhanced weight gain.
Vascular: The splenic and pancreaticoduodenal arteries provide blood to the pancreas.
The pancreaticoduodenal and splenic veins lead to the portal vein via venous drainage.
Investigations
Endoscopy/ERCP: histology and diagnosis.
Imaging: FDG-PET scans, endoscopic ultrasonography, angiography, CT, and MRCP for staging, diagnosis, and resectability evaluation.
FBC, U&E, LFT, CA19-9, and CEA in blood.
Pre-operative care may involve biliary decompression or stenting, blood and crossmatch, and multidisciplinary discussion. Use broad-spectrum antibiotics to cover.
Following surgery, post-operative treatment should include ICU/HDU supervision, insulin to regulate blood sugar, H2 receptor antagonists or proton pump inhibitors, octreotide and thromboprophylaxis, and, in the long run, pancreatic enzyme supplements. Perhaps adjuvant chemoradiotherapy is necessary.
Procedure
Supine position is used.
Rooftop, vertical midline, or transverse incisions are all possible.
Examination: Resectability of lesion and contents of abdomen assessed. Palliation via bypass, such as gastrojejunostomy and choledocho- or cholecystojejunostomy, if it is incurable.
Mobilization: In a pylorus-preserving surgery, the duodenum is mobilized (Kocherization) and the distal stomach is divided or the duodenum is divided 2 cm distal to the pylorus. Along with the gallbladder, common bile duct, and proximal pancreas, the duodenum is removed along with lymph nodes. To guarantee distinct margins during pancreatic resection, utilize frozen section. One can conduct an end-to-end or side-to-side pancreaticojejunostomy. An end-to-side pylorus-jejunotomy, end-to-side gastrojejunostomy, and end-to-side hepaticojejunostomy are made further downstream. You can create a feeding jejunostomy to provide nutritional support.
Conclusion: prudent hemostasis. The positioning of drains. Mass closure. Skin can be sealed using clips or subcuticular sutures.
Complications
The rate of morbidity is 40%. bleeding, dumping, reflux, anastomotic leak, biliary leak, ileus, hyperglycemia, sepsis from an abdomen or wound, delayed gastric emptying, pancreatitis, pancreatic fistula, and pancreatic insufficiency.
Prognosis
This is a significant surgical procedure that need to be carried out in specialized hospitals with current death rates around 5%. 30% of 5-year survival rates for resectable tumors.
0 Comments
