- Published on
Surgery- Parathyroid Disease
Introduction
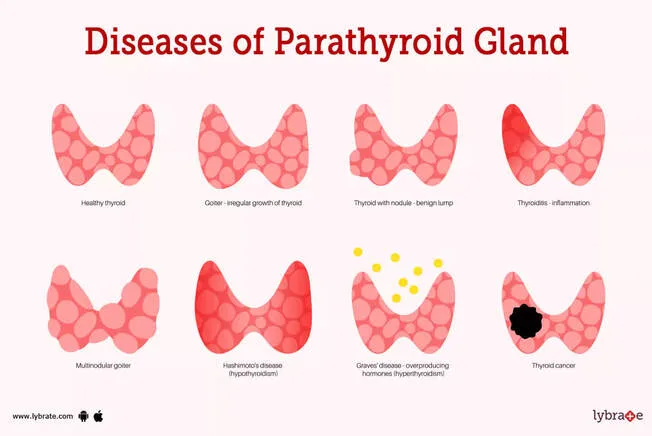
Primary hyperparathyroidism with hypercalcaemia and osteomalacia can be caused by benign parathyroid gland tumors (parathyroid adenomas) or parathyroid hyperplasia with excessive parathyroid hormone (PTH) release.
Malignancy (parathyroid adenocarcinomas) occurs seldom.
Etiology
It is uncertain exactly what causes these benign tumors to form. Past radiation exposure to the head, neck, and chest is linked to a higher risk of parathyroid adenomas.
One possible association between parathyroid adenomas and endocrine tumor syndromes is MENI and MENIIa.
Epidemiology
Seldom Used. One in a thousand, usually in the 50–70 age range.
History
frequently asymptomatic and detected by regular blood tests as hypercalcemia.
Hypercalcaemia symptoms could include:. weariness, arthralgia, and myalgia. bone ache. Nephrolithiasis. depression, anxiety, and diminished awareness. Pancreatitis
Other than the effects of hypercalcemia, an examination typically yields nothing.
Examination
Blood: bone profile (Ca2+, PTH), U&E (to evaluate fluid balance and electrolytes), plasma PTH.
Raised calcium levels in the urine.
Osteopenia and osteoporosis on plain radiographs. lesions in cystic bones.
To rule out sarcoidosis, use CXR.
Nuclear imaging: The location of the adenoma may be determined by technetium-99 scintigraphy.
US neck: Parathyroid adenomas may present differently.
To determine the severity of osteopenia or osteoporosis, a DEXA bone scan is required.
Management
IV rehydration with normal saline is the treatment for hypercalcemia. After rehydrating, keep up the fluid intake while using loop diuretics, such as furosemide, to improve renal calcium excretion.
Keep an eye on the other electrolytes. Take into account IV calcitonin, pamidronate (which increases bone resorption), or steroids (which are only useful in treating other causes of hypercalcaemia).
Surgery: Total parathyroidectomy (removal of all aberrant glands) and neck exploration.
Directed parathyroidectomy may be an option if the adenoma's location is well determined (requiring the use of more than one modality); alternatively, parathyroidectomy may be carried out under the guidance of intraoperative PTH level monitoring, since PTH levels begin to decline shortly after the adenoma is removed.
Complications
Surgical risks include the possibility of post-operative hypoparathyroidism from "hungry bone syndrome," which may necessitate temporary vitamin D and calcium supplements.
There is a significant danger of recurrent laryngeal nerve damage, particularly with thorough neck examination. Vocal cord paralysis can be detected by laryngoscopy, and some of the damage can be repaired partially by operating quickly to repair a severed nerve.
A large haematoma in the neck may need to be surgically removed in order to release the compressed trachea, which could compromise the airway.
consequences of hypercalcemia, such as osteoporosis, cognitive decline, and nephrolithiasis.
Good prognosis if the adenoma is completely removed. Many patients don't require any extra supplements.
Introduction
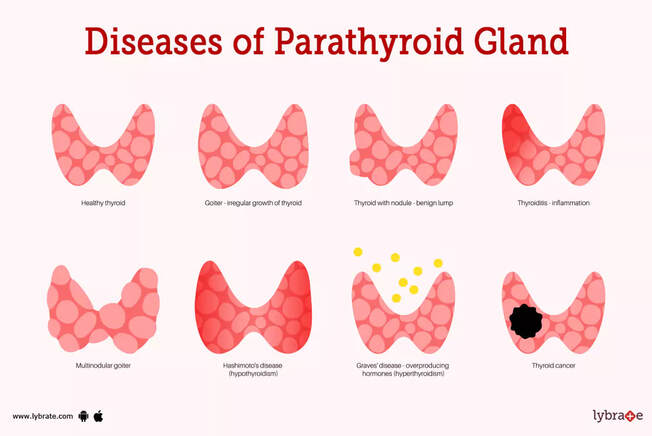
Primary hyperparathyroidism with hypercalcaemia and osteomalacia can be caused by benign parathyroid gland tumors (parathyroid adenomas) or parathyroid hyperplasia with excessive parathyroid hormone (PTH) release.
Malignancy (parathyroid adenocarcinomas) occurs seldom.
Etiology
It is uncertain exactly what causes these benign tumors to form. Past radiation exposure to the head, neck, and chest is linked to a higher risk of parathyroid adenomas.
One possible association between parathyroid adenomas and endocrine tumor syndromes is MENI and MENIIa.
Epidemiology
Seldom Used. One in a thousand, usually in the 50–70 age range.
History
frequently asymptomatic and detected by regular blood tests as hypercalcemia.
Hypercalcaemia symptoms could include:. weariness, arthralgia, and myalgia. bone ache. Nephrolithiasis. depression, anxiety, and diminished awareness. Pancreatitis
Other than the effects of hypercalcemia, an examination typically yields nothing.
Examination
Blood: bone profile (Ca2+, PTH), U&E (to evaluate fluid balance and electrolytes), plasma PTH.
Raised calcium levels in the urine.
Osteopenia and osteoporosis on plain radiographs. lesions in cystic bones.
To rule out sarcoidosis, use CXR.
Nuclear imaging: The location of the adenoma may be determined by technetium-99 scintigraphy.
US neck: Parathyroid adenomas may present differently.
To determine the severity of osteopenia or osteoporosis, a DEXA bone scan is required.
Management
IV rehydration with normal saline is the treatment for hypercalcemia. After rehydrating, keep up the fluid intake while using loop diuretics, such as furosemide, to improve renal calcium excretion.
Keep an eye on the other electrolytes. Take into account IV calcitonin, pamidronate (which increases bone resorption), or steroids (which are only useful in treating other causes of hypercalcaemia).
Surgery: Total parathyroidectomy (removal of all aberrant glands) and neck exploration.
Directed parathyroidectomy may be an option if the adenoma's location is well determined (requiring the use of more than one modality); alternatively, parathyroidectomy may be carried out under the guidance of intraoperative PTH level monitoring, since PTH levels begin to decline shortly after the adenoma is removed.
Complications
Surgical risks include the possibility of post-operative hypoparathyroidism from "hungry bone syndrome," which may necessitate temporary vitamin D and calcium supplements.
There is a significant danger of recurrent laryngeal nerve damage, particularly with thorough neck examination. Vocal cord paralysis can be detected by laryngoscopy, and some of the damage can be repaired partially by operating quickly to repair a severed nerve.
A large haematoma in the neck may need to be surgically removed in order to release the compressed trachea, which could compromise the airway.
consequences of hypercalcemia, such as osteoporosis, cognitive decline, and nephrolithiasis.
Good prognosis if the adenoma is completely removed. Many patients don't require any extra supplements.
0 Comments
