- Published on
Surgery - Penile Carcinoma
Introduction
The most frequent type of penile cancer is squamous cell carcinoma.
Etiology
The primary risk factor is :
-Human papillomavirus Condyloma acuminata & Balanitis, a persistent foreskin infection, and smoking
- Balanitis xerotica obliterans (a type of lichen sclerosus, a chronic inflammatory illness of the glans or foreskin);
-Bowen's disease (intraepithelial carcinoma of the penile shaft);
-Erythroplasia of Queyrat (a type of cancer in situ of the glans skin).
Epidemiology
In developed nations, uncommon (<0.5% of adult male cancer cases). more prevalent in South America and Africa. Most frequently observed in older men (aged 50–70).
History
The patient may describe a gradually growing lesion that is frequently painless, delaying seeking medical assistance. There can be discharge or bleeding in addition.
Examination
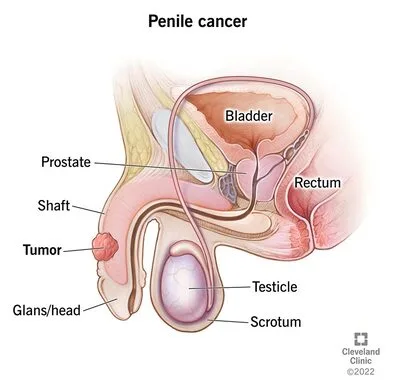
Most frequently appears on the inner surface of the foreskin or glans penis. It starts off as a painless red lesion and progresses to an exophytic or nodular growth or ulcer. A secondary infection that frequently results in a discharge or disagreeable odor is also common. Up to 50% of cases had inguinal lymphadenopathy, which is frequently brought on by an infection or inflammation, but only 30–60% of these cases show indications of tumor dissemination.
Pathogenesis
These are G1–G3 histological grades of squamous cell carcinomas. Jackson categorization of Stage I: Limited to the foreskin or glans. Stage II: The corpora's involvement.
Stage III: Inguinal nodes are reached. Remote metastases are in Stage IV. TNM staging is also included. Giant condyloma of Buschke-Lowenstein is a variation that exhibits a distinctive strongly defined deep boundary and spreads locally.
Investigations
Punch or excisional biopsy is used to make the diagnosis (condylomata acuminata, syphilitic chancre, or infrequently chancroid are the differential diagnoses).
Imaging: looking for signs of spread using CT or MRI scanning. biopsy of sentinal lymph nodes.
Management
Localized disease: 5-fluorouracil cream, laser photocoagulation, or cryosurgery for glans or Bowens disease on the shaft (carcinoma in situ).
Operative: Wide local excision, Mohs microsurgery, stage I and II, and partial penectomy with 2 cm proximal disease-free margins are recommended for the early stage. Complete penectomy combined with the creation of a perineal urethrostomy in more complex instances.
If impalpable, occult metastases occur in 20–25% of inguinal nodes. Metastases may not be the cause of palpable nodes. If a scanning results in suspicion, bilateral lymphadenectomy. More recently, limited inguinal node dissection superficial to the fascia lata or sentinel node biopsy.
Radiotherapy: As part of a combination modality therapy for the palliation of advanced-stage cancer, or locally for early-stage disease if the tumor is not big, invasive, or involves the urethra.
Chemotherapy: Usually limited to cases when the cancer has spread systemically; medications like cisplatin and irinotecan be utilized.
Prevention: The number of newborns who need to be circumcised to prevent one case of cancer is reduced by 909. Maintaining proper cleanliness and receiving the right care for Queyrat erythroplasia.
Complications
Following surgery: urethral stricture, wound disintegration, infection, and lymphoedema. Penectomy's psychological side effects.
Prognosis
frequently arrive late out of shame or neglect. The five-year survival rate for in situ disease is >90%; for invasive disease that has not progressed to lymph nodes, it is 80%; for nodal involvement, it is roughly 50%; and for distant metastases, it is less than 20%.
Introduction
The most frequent type of penile cancer is squamous cell carcinoma.
Etiology
The primary risk factor is :
-Human papillomavirus Condyloma acuminata & Balanitis, a persistent foreskin infection, and smoking
- Balanitis xerotica obliterans (a type of lichen sclerosus, a chronic inflammatory illness of the glans or foreskin);
-Bowen's disease (intraepithelial carcinoma of the penile shaft);
-Erythroplasia of Queyrat (a type of cancer in situ of the glans skin).
Epidemiology
In developed nations, uncommon (<0.5% of adult male cancer cases). more prevalent in South America and Africa. Most frequently observed in older men (aged 50–70).
History
The patient may describe a gradually growing lesion that is frequently painless, delaying seeking medical assistance. There can be discharge or bleeding in addition.
Examination
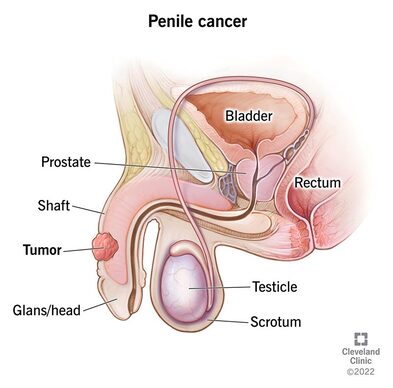
Most frequently appears on the inner surface of the foreskin or glans penis. It starts off as a painless red lesion and progresses to an exophytic or nodular growth or ulcer. A secondary infection that frequently results in a discharge or disagreeable odor is also common. Up to 50% of cases had inguinal lymphadenopathy, which is frequently brought on by an infection or inflammation, but only 30–60% of these cases show indications of tumor dissemination.
Pathogenesis
These are G1–G3 histological grades of squamous cell carcinomas. Jackson categorization of Stage I: Limited to the foreskin or glans. Stage II: The corpora's involvement.
Stage III: Inguinal nodes are reached. Remote metastases are in Stage IV. TNM staging is also included. Giant condyloma of Buschke-Lowenstein is a variation that exhibits a distinctive strongly defined deep boundary and spreads locally.
Investigations
Punch or excisional biopsy is used to make the diagnosis (condylomata acuminata, syphilitic chancre, or infrequently chancroid are the differential diagnoses).
Imaging: looking for signs of spread using CT or MRI scanning. biopsy of sentinal lymph nodes.
Management
Localized disease: 5-fluorouracil cream, laser photocoagulation, or cryosurgery for glans or Bowens disease on the shaft (carcinoma in situ).
Operative: Wide local excision, Mohs microsurgery, stage I and II, and partial penectomy with 2 cm proximal disease-free margins are recommended for the early stage. Complete penectomy combined with the creation of a perineal urethrostomy in more complex instances.
If impalpable, occult metastases occur in 20–25% of inguinal nodes. Metastases may not be the cause of palpable nodes. If a scanning results in suspicion, bilateral lymphadenectomy. More recently, limited inguinal node dissection superficial to the fascia lata or sentinel node biopsy.
Radiotherapy: As part of a combination modality therapy for the palliation of advanced-stage cancer, or locally for early-stage disease if the tumor is not big, invasive, or involves the urethra.
Chemotherapy: Usually limited to cases when the cancer has spread systemically; medications like cisplatin and irinotecan be utilized.
Prevention: The number of newborns who need to be circumcised to prevent one case of cancer is reduced by 909. Maintaining proper cleanliness and receiving the right care for Queyrat erythroplasia.
Complications
Following surgery: urethral stricture, wound disintegration, infection, and lymphoedema. Penectomy's psychological side effects.
Prognosis
frequently arrive late out of shame or neglect. The five-year survival rate for in situ disease is >90%; for invasive disease that has not progressed to lymph nodes, it is 80%; for nodal involvement, it is roughly 50%; and for distant metastases, it is less than 20%.
0 Comments
