- Published on
Surgery - Peritonitis
Introduction
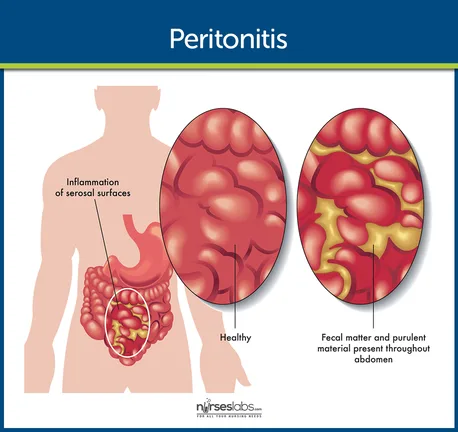
Inflammation of the abdominal cavity's peritoneal lining is known as peritonitis, and it can be either localized or widespread, with the latter being either primary or secondary.
Etiology
Localized: Cholecystitis, diverticulitis, appendicitis, and salpingitis are common causes.
Primary generalized: Peritoneal cavity infection caused by bacteria that isn't clearly focused on one area. Children may develop primary pneumococcal peritonitis as a result of Streptococcus penumoniae. In adults, frequently linked to renal failure patients receiving CAPD (continuous ambulatory peritoneal dialysis) or cirrhosis and ascites (spontaneous bacterial peritonitis).
Secondary generalized: Peptic ulcers, ruptured peptic ulcers, pancreatic discharges (a chemical kind of peritonitis that frequently becomes secondary infected), and other localized infective foci that are either polymicrobial (see above) or nonbacterial.
Epidemiology
While secondary generalized and localized peritonitis are more common, primary peritonitis is uncommon and typically manifests in adolescent females.
History
A thorough history should be obtained, covering the genesis, character, progression, and dissemination of the abdominal pain in addition to aggravating, mitigating, and concomitant events. As a result of movement and coughing, parietal pain from peritonitis is typically constant, intense, localized, and made worse (parietal peritoneum is supplied by somatic A-d fibres emanating from spinal neurons of T7–L2).
Examination
Examine vital signs, indicators of dehydration, and evidence of reduced perfusion (from hypovolemia, sepsis, or circulatory failure, for example).
Regionalized: Tenderness accompanied with involuntary guarding: reflex contraction of the muscles covering the abdominal wall; rebound tenderness: pain resulting from the inflamed peritoneum moving when a palpating hand is suddenly removed; this is also exhibited by percussion tenderness or pain triggered by coughing.
Generalized: Movement makes the patient's discomfort worse; they are typically extremely ill with systemic symptoms of toxaemia or sepsis (such as fever, tachycardia). Due to paralytic ileus, the belly is rigid with widespread rebound and guarding, and bowel sounds are either attenuated or usually nonexistent.
Investigational studies
as demonstrated by the clinical evaluation and history.
Blood tests include FBC, U&Es, LFT, amylase, CRP, coagulation, G&S or crossmatch, blood cultures, and ABG (which looks for respiratory failure, lactate accumulation, or metabolic acidosis).
For pneumoperitoneum, erect CXR.
AXR: For blockage of the bowel.
Laparoscopy or CT abdomen: To identify the peritonitis's etiology. The peritoneum becomes erythematous and loses its glossy aspect when it is inflamed. This is due to the creation of a large amount of serous inflammatory exudate, which is rich in protein, inflammatory mediators, and white blood cells. The larger omentum adheres to the irritated organ, preventing the infection from spreading.
If ascites: Gram stain, culture, ascitic tap and cell count (diagnostic of SBP if >250 neutrophils/mm3).
Management
Localized: The course of treatment will be determined by the underlying cause (appendicitis, for example), as well as IV antibiotics (cholecystitis, salpingitis, and the majority of cases of acute diverticulitis).
Generalized: Sepsis and shock could cause the patient to die. Requires IV fluid replacement, volume and electrolyte imbalance correction, and IV antibiotics. CVP line, NG tube, and urinary catheter to track fluid balance and determine the need for surgery.
Emergency laparotomy/laparoscopy: To determine the cause, treat it, remove any necrotic or infected tissue, and make a large amount of peritoneal lavage. An acute non-necrotizing pancreatitis would be an exception.
Antibiotics are used to treat primary peritonitis, but this diagnosis is frequently made only after an effort at surgical intervention has been made.
Complications
Early: Portal pyaemia/hepatic abscesses, wound infection, tertiary peritonitis (persistence of intra-abdominal infection), paralytic ileus, septic shock, respiratory or multi-organ failure.
Late: adhesions and incisional hernia.
Prognosis
Localized peritonitis typically goes away when the underlying cause is treated appropriately.
The mortality rate for generalized peritonitis is substantially higher, at about 30–50%. The death rate may rise to more than 70% if septic shock or multi-organ failure develops concurrently.
With the right antibiotic therapy, the prognosis for primary peritonitis is favorable. Patients with SBP may have a total mortality risk of more than 30% if diagnosis and treatment are put off.
Introduction
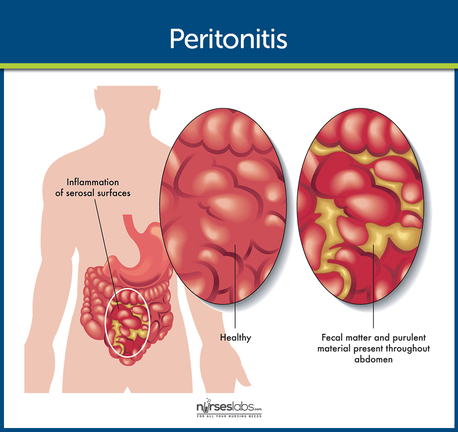
Inflammation of the abdominal cavity's peritoneal lining is known as peritonitis, and it can be either localized or widespread, with the latter being either primary or secondary.
Etiology
Localized: Cholecystitis, diverticulitis, appendicitis, and salpingitis are common causes.
Primary generalized: Peritoneal cavity infection caused by bacteria that isn't clearly focused on one area. Children may develop primary pneumococcal peritonitis as a result of Streptococcus penumoniae. In adults, frequently linked to renal failure patients receiving CAPD (continuous ambulatory peritoneal dialysis) or cirrhosis and ascites (spontaneous bacterial peritonitis).
Secondary generalized: Peptic ulcers, ruptured peptic ulcers, pancreatic discharges (a chemical kind of peritonitis that frequently becomes secondary infected), and other localized infective foci that are either polymicrobial (see above) or nonbacterial.
Epidemiology
While secondary generalized and localized peritonitis are more common, primary peritonitis is uncommon and typically manifests in adolescent females.
History
A thorough history should be obtained, covering the genesis, character, progression, and dissemination of the abdominal pain in addition to aggravating, mitigating, and concomitant events. As a result of movement and coughing, parietal pain from peritonitis is typically constant, intense, localized, and made worse (parietal peritoneum is supplied by somatic A-d fibres emanating from spinal neurons of T7–L2).
Examination
Examine vital signs, indicators of dehydration, and evidence of reduced perfusion (from hypovolemia, sepsis, or circulatory failure, for example).
Regionalized: Tenderness accompanied with involuntary guarding: reflex contraction of the muscles covering the abdominal wall; rebound tenderness: pain resulting from the inflamed peritoneum moving when a palpating hand is suddenly removed; this is also exhibited by percussion tenderness or pain triggered by coughing.
Generalized: Movement makes the patient's discomfort worse; they are typically extremely ill with systemic symptoms of toxaemia or sepsis (such as fever, tachycardia). Due to paralytic ileus, the belly is rigid with widespread rebound and guarding, and bowel sounds are either attenuated or usually nonexistent.
Investigational studies
as demonstrated by the clinical evaluation and history.
Blood tests include FBC, U&Es, LFT, amylase, CRP, coagulation, G&S or crossmatch, blood cultures, and ABG (which looks for respiratory failure, lactate accumulation, or metabolic acidosis).
For pneumoperitoneum, erect CXR.
AXR: For blockage of the bowel.
Laparoscopy or CT abdomen: To identify the peritonitis's etiology. The peritoneum becomes erythematous and loses its glossy aspect when it is inflamed. This is due to the creation of a large amount of serous inflammatory exudate, which is rich in protein, inflammatory mediators, and white blood cells. The larger omentum adheres to the irritated organ, preventing the infection from spreading.
If ascites: Gram stain, culture, ascitic tap and cell count (diagnostic of SBP if >250 neutrophils/mm3).
Management
Localized: The course of treatment will be determined by the underlying cause (appendicitis, for example), as well as IV antibiotics (cholecystitis, salpingitis, and the majority of cases of acute diverticulitis).
Generalized: Sepsis and shock could cause the patient to die. Requires IV fluid replacement, volume and electrolyte imbalance correction, and IV antibiotics. CVP line, NG tube, and urinary catheter to track fluid balance and determine the need for surgery.
Emergency laparotomy/laparoscopy: To determine the cause, treat it, remove any necrotic or infected tissue, and make a large amount of peritoneal lavage. An acute non-necrotizing pancreatitis would be an exception.
Antibiotics are used to treat primary peritonitis, but this diagnosis is frequently made only after an effort at surgical intervention has been made.
Complications
Early: Portal pyaemia/hepatic abscesses, wound infection, tertiary peritonitis (persistence of intra-abdominal infection), paralytic ileus, septic shock, respiratory or multi-organ failure.
Late: adhesions and incisional hernia.
Prognosis
Localized peritonitis typically goes away when the underlying cause is treated appropriately.
The mortality rate for generalized peritonitis is substantially higher, at about 30–50%. The death rate may rise to more than 70% if septic shock or multi-organ failure develops concurrently.
With the right antibiotic therapy, the prognosis for primary peritonitis is favorable. Patients with SBP may have a total mortality risk of more than 30% if diagnosis and treatment are put off.
0 Comments
