- Published on
Surgery - Pulmonary Embolism
Introduction
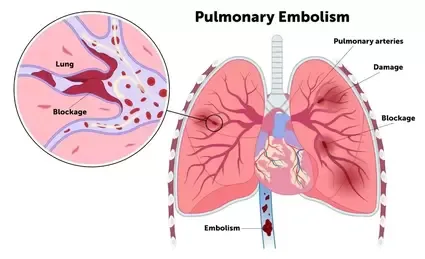
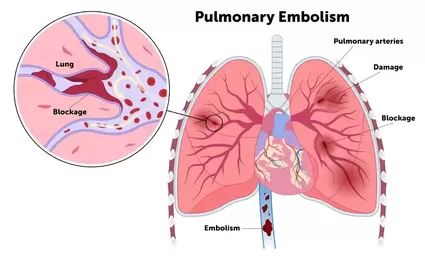
blockage of the pulmonary arteries, usually caused by a thrombus that entered the system from another location.
Etiology
Thrombus (rarely from the right atrium in patients with atrial fibrillation, and more than 95% originating from DVT of the lower limbs). A variety of substances, such as amniotic fluid, air, fat, tumors, and mycotic emboli from right-sided endocarditis, can also embolise to pulmonary arteries. Patients undergoing surgery, as well as those with immobility, obesity, OCP, heart failure, or cancer, are among the groups most at risk.
Epidemiology
very common, particularly in hospitalized patients; affect 10–20% of individuals with proximal DVT that has been verified.
History
Depending on the pulmonary embolus's size and location. Minimal: Could show no symptoms. Moderate: Cough, hemoptysis, pleuritic chest discomfort, and sudden onset dyspnea. Large (or proximal): All of the previous symptoms plus abrupt death, shock, collapse, acute right heart failure, or severe central pleuritic chest discomfort. Pulmonary hypertension symptoms include multiple minor recurring episodes.
Examination
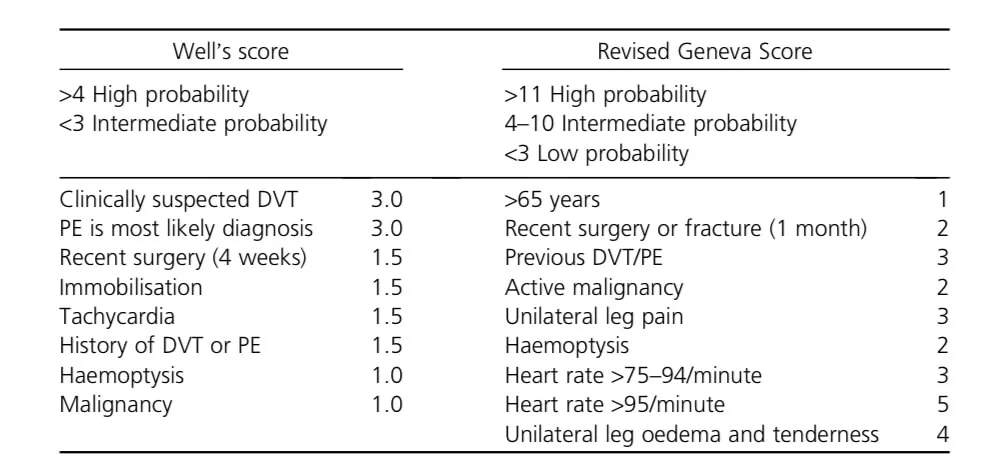
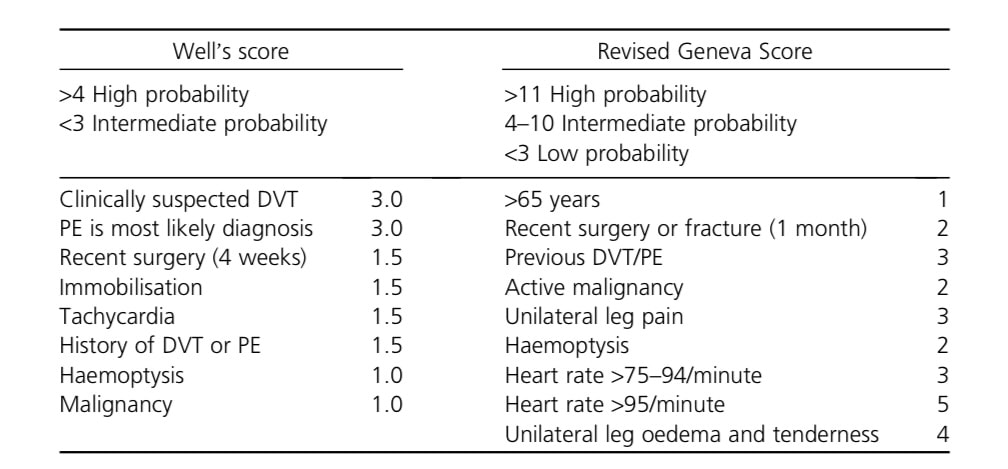
Evaluation of clinical probability: Different scores can be used to estimate probability and direct management and additional research. Apply regional regulations.
Introduction
blockage of the pulmonary arteries, usually caused by a thrombus that entered the system from another location.
Etiology
Thrombus (rarely from the right atrium in patients with atrial fibrillation, and more than 95% originating from DVT of the lower limbs). A variety of substances, such as amniotic fluid, air, fat, tumors, and mycotic emboli from right-sided endocarditis, can also embolise to pulmonary arteries. Patients undergoing surgery, as well as those with immobility, obesity, OCP, heart failure, or cancer, are among the groups most at risk.
Epidemiology
very common, particularly in hospitalized patients; affect 10–20% of individuals with proximal DVT that has been verified.
History
Depending on the pulmonary embolus's size and location. Minimal: Could show no symptoms. Moderate: Cough, hemoptysis, pleuritic chest discomfort, and sudden onset dyspnea. Large (or proximal): All of the previous symptoms plus abrupt death, shock, collapse, acute right heart failure, or severe central pleuritic chest discomfort. Pulmonary hypertension symptoms include multiple minor recurring episodes.
Examination
Evaluation of clinical probability: Different scores can be used to estimate probability and direct management and additional research. Apply regional regulations.
Investigational studies
Low probability: Use the blood test known as the D-dimer (sensitive but insensitive to cross-linked fibrin breakdown products). High probability: Imaging is necessary. Further preliminary inquiries: Blood: Think of a thrombophilia screen, ABG. ECG: May be normal, however tachycardia, right axis deviation, or RBBB are more frequently seen. Classical patterns such as SI, QIII, or TIII are not very prevalent. CXR: Usually normal, but check for other differential diagnosis. Spiral CT pulmonary angiogram: The preferred initial diagnostic procedure. Very sensitive for medium-to large-sized emboli, but poor sensitivity for tiny emboli. Inhaling krypton-81 gas and administering IV 99mTc macro-aggregated albumin constitute the ventilation-perfusion (VQ) scan. This shows where there may be a mismatch between perfusion and ventilation. Not appropriate because to interpretation difficulties if there is a concurrent lung disease or an abnormal CXR. The gold standard for pulmonary angiography is invasive. seldom required. To check for venous thrombosis, do a lower limb Doppler ultrasound. Right heart strain may be seen on an echocardiogram.
Management
Primary prevention: Heparin prophylaxis in at-risk individuals (e.g., those undergoing surgery) and graduated pressure stockings (TEDs). prompt mobilization and sufficient hydration following surgery. If the patient's blood pressure is stable, they should start on O2, anticoagulate with heparin or LMW heparin, and switch to oral warfarin medication (INR 2-3) for at least three months. drugs that reduce pain. If hemodynamically unstable (massive PE): If cardiac arrest is likely, resuscitate, provide oxygen, IV fluid resuscitation, and thrombolysis with tissue plasminogen activator (tPA) may be considered solely on the basis of clinical considerations. Embolectomy, either surgical or radiological (where thrombolysis is contraindicated). When anticoagulation is contraindicated or for recurrent pulmonary emboli, IVC filters (such as the Greenfield filter) may be placed.
Complications
Right heart failure, pulmonary hypertension, death, and pulmonary infarction.
Prognosis
30% of deaths go untreated, 8% are treated (because of recurring emboli or underlying disease). "Risk of future thrombo-embolic disease" is present in patients.
Low probability: Use the blood test known as the D-dimer (sensitive but insensitive to cross-linked fibrin breakdown products). High probability: Imaging is necessary. Further preliminary inquiries: Blood: Think of a thrombophilia screen, ABG. ECG: May be normal, however tachycardia, right axis deviation, or RBBB are more frequently seen. Classical patterns such as SI, QIII, or TIII are not very prevalent. CXR: Usually normal, but check for other differential diagnosis. Spiral CT pulmonary angiogram: The preferred initial diagnostic procedure. Very sensitive for medium-to large-sized emboli, but poor sensitivity for tiny emboli. Inhaling krypton-81 gas and administering IV 99mTc macro-aggregated albumin constitute the ventilation-perfusion (VQ) scan. This shows where there may be a mismatch between perfusion and ventilation. Not appropriate because to interpretation difficulties if there is a concurrent lung disease or an abnormal CXR. The gold standard for pulmonary angiography is invasive. seldom required. To check for venous thrombosis, do a lower limb Doppler ultrasound. Right heart strain may be seen on an echocardiogram.
Management
Primary prevention: Heparin prophylaxis in at-risk individuals (e.g., those undergoing surgery) and graduated pressure stockings (TEDs). prompt mobilization and sufficient hydration following surgery. If the patient's blood pressure is stable, they should start on O2, anticoagulate with heparin or LMW heparin, and switch to oral warfarin medication (INR 2-3) for at least three months. drugs that reduce pain. If hemodynamically unstable (massive PE): If cardiac arrest is likely, resuscitate, provide oxygen, IV fluid resuscitation, and thrombolysis with tissue plasminogen activator (tPA) may be considered solely on the basis of clinical considerations. Embolectomy, either surgical or radiological (where thrombolysis is contraindicated). When anticoagulation is contraindicated or for recurrent pulmonary emboli, IVC filters (such as the Greenfield filter) may be placed.
Complications
Right heart failure, pulmonary hypertension, death, and pulmonary infarction.
Prognosis
30% of deaths go untreated, 8% are treated (because of recurring emboli or underlying disease). "Risk of future thrombo-embolic disease" is present in patients.
0 Comments
