- Published on
Surgery - Renal Transplantation
Indications
Dialysis is necessary for end-stage renal failure (creatinine clearance <20 ml/min) or is expected to be necessary in the next six to twelve months. The most frequent causes are renovascular disease, polycystic kidney disease, reflux nephropathy, glomerulonephritis, diabetic nephropathy, and hypertension.
When compared to dialysis, renal transplantation is more affordable and increases life expectancy.
Anatomy
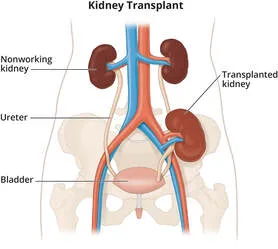
The donor kidney is implanted heterotopically, that is, retroperitoneally in the iliac fossa, but not in the same spot as the native kidney. Renal vessels are anastomosed to the IVC and aorta in adults, and occasionally to the external iliac arteries in infants. The bladder and ureter are anastomosed. Because the connecting vein and artery are longer, transplanting left kidneys typically presents less of a challenge.
Unless they provide a risk of recurrent infections or, in the case of large polycystic kidneys, impinge into the iliac fossa, native kidneys are typically left in situ.
Investigations
Workup before to surgery: Multidisciplinary evaluation, such as echocardiography, angiography, perfusion investigations, or ECG, should include cardiovascular evaluation since dialysis patients frequently have ischemic heart disease. HIV, hepatitis B, C, EBV, CMV, and other viral screens.
Donors who are alive: can be altruistic, unrelated, or related donors, and they all need a comprehensive medical and psychological evaluation. people in good health with typical renal function. Angiography (CT or MR) can be used to examine the anatomy of the renal vessels.
Tissue typing and panel-reactive antibody titres: An enhanced result is obtained by better matching of the major histocompatibility loci, class II DR > class I B > class I A. Patients on the waiting list, as well as lymphocytes from the spleen or donor lymph node, are subjected to HLA typing. A nationwide organ-sharing network facilitates the quick identification of the most appropriate recipient by identifying identical or "favourable" matches. Blood group compatibility of donor kidneys is ensured, and recipients undergo screening for antibodies that may cause hyperacute rejection. The possibility that a kidney donor selected at random will have a positive cytotoxic lymphocyte crossmatch with the intended recipient is estimated by the titre of the panel-reactive antibody.
Actions
Organ donation: In the UK, only 20% of patients have an eligible living donor; the remaining organs come from cadavers. In every situation, the next of kin gives their consent. Donors should be free of cancer (except from primary brain tumors), have good renal function, and undergo screening for hepatitis, HIV, and CMV.
Organ retrieval: In order to minimize heated ischaemia time, the kidneys are removed as part of a multi-organ retrieval procedure. They are then in situ perfused with a cold preservative solution, such as the Marshall or University of Wisconsin solution. The kidney is removed with perinephric fat in situ to prevent injury. While less than 24 hours is acceptable, preservation times should be kept to a minimum since any more can increase the likelihood of both short- and long-term failure. Machine cold perfusion of cadaveric kidneys has been demonstrated in trials to improve graft survival and decrease delayed graft function.
Recipient operation: An extraperitoneal technique using an oblique lower abdominal incision provides access to the bladder and iliac veins. Following the anastomosis of the renal vein to the external iliac vein, an end-to-side arterial anastomosis is typically formed, frequently utilizing a donor aortic patch (Carrel patch). Next, a ureteric stent is used to produce a ureteroneocystostomy. For a few days, an indwelling catheter is left in place to allow the bladder incision to heal. Immunosuppression is started and antibiotic prophylaxis is administered. Fluid balance needs to be closely monitored after surgery.
Immunosuppression: Immune risk levels are categorized as low or high, for example, diabetes risk associated with a second transplant (new-onset diabetes after transplantation, or NODAT).
Medications include corticosteroids, monoclonal antibodies, calcineurin inhibitors (like tacrolimus and cyclosporin), purine synthesis inhibitors (like azathioprine and mycophenolate mofetil), and monoclonal antibodies (like basiliximab, an IL-2 receptor antagonist). Renal function deterioration is examined by biopsies, Doppler, and ultrasonography.
Complications
Impaired graft function: Twenty to thirty percent of cases of acute tubular necrosis result in delayed graft function.
Vascular (1%–5%): renal vein thrombosis, renal artery thrombosis, renal artery stenosis, and hemorrhage.
Urological (2–10%): reflux, ureteric stenosis (managed with ureteroplasty, stent placement, or open surgery), bladder leak, and ureteric leak.
Lymphocoeles: Caused by disruption of lymphatics, occurring in 1-6 percent of transplants; treated by marsupialization into the peritoneum or percutaneous drainage.
Early infection: infections caused by bacteria. Subsequent: Opportunistic infections, such as Candida, CMV, BK virus, HSV, and Pneumocystis.
Rejection: . Excessive: Owing to already-formed antibodies.
Crossmatching before transplantation ought to stop this from happening.
Acute: Up to 40% of cases are most common. because of T-cells attacking the graft, which was treated with steroid boluses or antibody therapy when renal function abnormalities and a kidney biopsy revealed the attack.
Chronic: A late-onset renal disease characterized by progressive loss of renal function, proteinuria, and hypertension. resistant to the majority of treatments and finally lead to graft failure.
Immunosuppression includes drug side effects, infections, and post-transplant cancers, such as an increased risk of skin cancer and lymphomas (a condition known as post-transplant lymphoproliferative illness).
Patient survival was >90% at one year and >80% at five years for PRONOS I S. Overall graft survival was 85% for cadaveric donors and 90–95% for living donors at 12 months. After that, 3-5 percent of grafts were lost annually.
Following a transplant, cardiovascular problems account for the majority of deaths.
Indications
Dialysis is necessary for end-stage renal failure (creatinine clearance <20 ml/min) or is expected to be necessary in the next six to twelve months. The most frequent causes are renovascular disease, polycystic kidney disease, reflux nephropathy, glomerulonephritis, diabetic nephropathy, and hypertension.
When compared to dialysis, renal transplantation is more affordable and increases life expectancy.
Anatomy
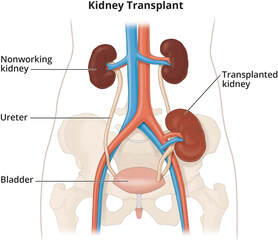
The donor kidney is implanted heterotopically, that is, retroperitoneally in the iliac fossa, but not in the same spot as the native kidney. Renal vessels are anastomosed to the IVC and aorta in adults, and occasionally to the external iliac arteries in infants. The bladder and ureter are anastomosed. Because the connecting vein and artery are longer, transplanting left kidneys typically presents less of a challenge.
Unless they provide a risk of recurrent infections or, in the case of large polycystic kidneys, impinge into the iliac fossa, native kidneys are typically left in situ.
Investigations
Workup before to surgery: Multidisciplinary evaluation, such as echocardiography, angiography, perfusion investigations, or ECG, should include cardiovascular evaluation since dialysis patients frequently have ischemic heart disease. HIV, hepatitis B, C, EBV, CMV, and other viral screens.
Donors who are alive: can be altruistic, unrelated, or related donors, and they all need a comprehensive medical and psychological evaluation. people in good health with typical renal function. Angiography (CT or MR) can be used to examine the anatomy of the renal vessels.
Tissue typing and panel-reactive antibody titres: An enhanced result is obtained by better matching of the major histocompatibility loci, class II DR > class I B > class I A. Patients on the waiting list, as well as lymphocytes from the spleen or donor lymph node, are subjected to HLA typing. A nationwide organ-sharing network facilitates the quick identification of the most appropriate recipient by identifying identical or "favourable" matches. Blood group compatibility of donor kidneys is ensured, and recipients undergo screening for antibodies that may cause hyperacute rejection. The possibility that a kidney donor selected at random will have a positive cytotoxic lymphocyte crossmatch with the intended recipient is estimated by the titre of the panel-reactive antibody.
Actions
Organ donation: In the UK, only 20% of patients have an eligible living donor; the remaining organs come from cadavers. In every situation, the next of kin gives their consent. Donors should be free of cancer (except from primary brain tumors), have good renal function, and undergo screening for hepatitis, HIV, and CMV.
Organ retrieval: In order to minimize heated ischaemia time, the kidneys are removed as part of a multi-organ retrieval procedure. They are then in situ perfused with a cold preservative solution, such as the Marshall or University of Wisconsin solution. The kidney is removed with perinephric fat in situ to prevent injury. While less than 24 hours is acceptable, preservation times should be kept to a minimum since any more can increase the likelihood of both short- and long-term failure. Machine cold perfusion of cadaveric kidneys has been demonstrated in trials to improve graft survival and decrease delayed graft function.
Recipient operation: An extraperitoneal technique using an oblique lower abdominal incision provides access to the bladder and iliac veins. Following the anastomosis of the renal vein to the external iliac vein, an end-to-side arterial anastomosis is typically formed, frequently utilizing a donor aortic patch (Carrel patch). Next, a ureteric stent is used to produce a ureteroneocystostomy. For a few days, an indwelling catheter is left in place to allow the bladder incision to heal. Immunosuppression is started and antibiotic prophylaxis is administered. Fluid balance needs to be closely monitored after surgery.
Immunosuppression: Immune risk levels are categorized as low or high, for example, diabetes risk associated with a second transplant (new-onset diabetes after transplantation, or NODAT).
Medications include corticosteroids, monoclonal antibodies, calcineurin inhibitors (like tacrolimus and cyclosporin), purine synthesis inhibitors (like azathioprine and mycophenolate mofetil), and monoclonal antibodies (like basiliximab, an IL-2 receptor antagonist). Renal function deterioration is examined by biopsies, Doppler, and ultrasonography.
Complications
Impaired graft function: Twenty to thirty percent of cases of acute tubular necrosis result in delayed graft function.
Vascular (1%–5%): renal vein thrombosis, renal artery thrombosis, renal artery stenosis, and hemorrhage.
Urological (2–10%): reflux, ureteric stenosis (managed with ureteroplasty, stent placement, or open surgery), bladder leak, and ureteric leak.
Lymphocoeles: Caused by disruption of lymphatics, occurring in 1-6 percent of transplants; treated by marsupialization into the peritoneum or percutaneous drainage.
Early infection: infections caused by bacteria. Subsequent: Opportunistic infections, such as Candida, CMV, BK virus, HSV, and Pneumocystis.
Rejection: . Excessive: Owing to already-formed antibodies.
Crossmatching before transplantation ought to stop this from happening.
Acute: Up to 40% of cases are most common. because of T-cells attacking the graft, which was treated with steroid boluses or antibody therapy when renal function abnormalities and a kidney biopsy revealed the attack.
Chronic: A late-onset renal disease characterized by progressive loss of renal function, proteinuria, and hypertension. resistant to the majority of treatments and finally lead to graft failure.
Immunosuppression includes drug side effects, infections, and post-transplant cancers, such as an increased risk of skin cancer and lymphomas (a condition known as post-transplant lymphoproliferative illness).
Patient survival was >90% at one year and >80% at five years for PRONOS I S. Overall graft survival was 85% for cadaveric donors and 90–95% for living donors at 12 months. After that, 3-5 percent of grafts were lost annually.
Following a transplant, cardiovascular problems account for the majority of deaths.
0 Comments
