- Published on
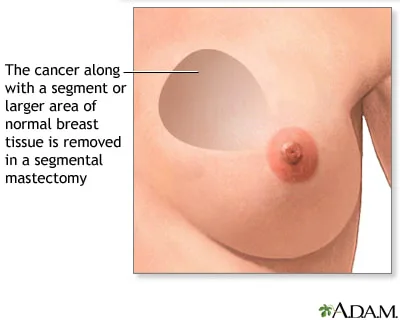
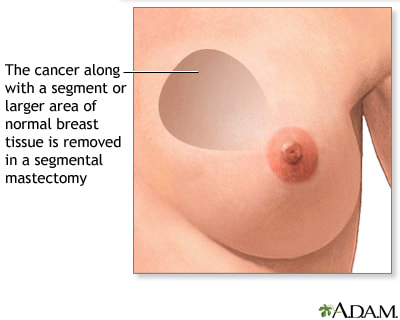
Surgery - Segmental Mastectomy (wide local excision)
Indications
One primary breast tumor that is excisable and has distinct resection margins (generally <4 cm with 1 cm margins). The patient needs to be a good candidate for follow-up and postoperative radiation.
Anatomy
There is a complex network of branching milk ducts that exit on the nipple (from 4 to 18 ducts; the anatomy originally reported by Cooper has been substantially changed in recent years). The breast tissue is composed of fatty and glandular tissue (ratio ranges from 1: 1 to 1: 2 in lactation). With an axillary tail, the base of the breast encloses the second through sixth ribs. Suspensory connective tissue ligaments support the breast tissue by extending from the dermis to the deep fascia.
Vascular: The internal mammary, intercostal, thoracodorsal, lateral thoracic, and thoracoacromial arteries, as well as their perforating arteries, provide the breast's arterial supply and associated venous drainage.
Lymphatics: The medial half drains into the nodes along the internal mammary artery, and the lateral half drains into the axillary nodes, which are made up of the anterior, posterior, lateral, central, and apical groups.
Investigations
Preoperative evaluation involves three methods: clinical examination, imaging (MRI, mammography, or ultrasound), and cytological investigation (FNA or trucut biopsy). Prior to surgery, imaging-guided wire localization can be necessary for smaller, impalpable lesions.
Tests for blood: FBC, U&Es, G&S, CXR, and ECG as necessary. general evaluation of anesthesia.
Prophylactic DVT after surgery. workouts for the shoulders to avoid stiffness, particularly following axillary surgery.
Procedure
Access: It is important to plan a skin incision that will look good visually. Transverse, circumferential, circumareolar, and inframammary are the available options. Skin excision is typically not necessary unless it is necessary to provide a sufficient margin free of tumors.
Excision: To remove the breast tissue containing the lesion with sufficient margins, dissection is carried out. Sutures should be used to mark the specimen so that histological investigation can be done with precise orientation. To ensure total excision of the lesion in wire-guided cases, an X-ray is taken of the specimen. To restore breast shape, it could be necessary to mobilize breast tissue. Haemostasis needs to be done carefully.
Closure: Usually, the skin and subcutaneous tissue layers are closed together.
A secondary incision is typically made behind the lateral border of the pectoralis major in order to perform the axillary node biopsy, sample, and clearing. Patients whose axilla is not clinically involved can benefit from sentinal node biopsy. Before surgery, radioactive tracer is injected into the breast, then on the day of the procedure, blue dye (methylene blue) is injected. To facilitate histological examination, the initial draining nodes are located and excised. Usually, an axillary clearing is carried out if there are implicated nodes. The pectoralis minor is used to determine the levels of axillary clearance, with level 1 nodes up to the muscle, level II nodes behind it, and level III nodes beyond the subclavius. The axillary vessels, thoracodorsal nerve and vessels (supply latissimus dorsi), and the long thoracic nerve of Bell (to serratus anterior) should be carefully dissected. The intercostobrachial nerve, which passes laterally through the axilla, may need to be sacrificed. Usually, a drain is left in place after clearing.
Complications
bleeding, seroma, infection, and inadequate cosmesis. following axillary surgery: winged scapula (long thoracic nerve injury), frozen shoulder, discomfort, lymphoedema, and numbness (intercostobrachial nerve injury).
Indications
One primary breast tumor that is excisable and has distinct resection margins (generally <4 cm with 1 cm margins). The patient needs to be a good candidate for follow-up and postoperative radiation.
Anatomy
There is a complex network of branching milk ducts that exit on the nipple (from 4 to 18 ducts; the anatomy originally reported by Cooper has been substantially changed in recent years). The breast tissue is composed of fatty and glandular tissue (ratio ranges from 1: 1 to 1: 2 in lactation). With an axillary tail, the base of the breast encloses the second through sixth ribs. Suspensory connective tissue ligaments support the breast tissue by extending from the dermis to the deep fascia.
Vascular: The internal mammary, intercostal, thoracodorsal, lateral thoracic, and thoracoacromial arteries, as well as their perforating arteries, provide the breast's arterial supply and associated venous drainage.
Lymphatics: The medial half drains into the nodes along the internal mammary artery, and the lateral half drains into the axillary nodes, which are made up of the anterior, posterior, lateral, central, and apical groups.
Investigations
Preoperative evaluation involves three methods: clinical examination, imaging (MRI, mammography, or ultrasound), and cytological investigation (FNA or trucut biopsy). Prior to surgery, imaging-guided wire localization can be necessary for smaller, impalpable lesions.
Tests for blood: FBC, U&Es, G&S, CXR, and ECG as necessary. general evaluation of anesthesia.
Prophylactic DVT after surgery. workouts for the shoulders to avoid stiffness, particularly following axillary surgery.
Procedure
Access: It is important to plan a skin incision that will look good visually. Transverse, circumferential, circumareolar, and inframammary are the available options. Skin excision is typically not necessary unless it is necessary to provide a sufficient margin free of tumors.
Excision: To remove the breast tissue containing the lesion with sufficient margins, dissection is carried out. Sutures should be used to mark the specimen so that histological investigation can be done with precise orientation. To ensure total excision of the lesion in wire-guided cases, an X-ray is taken of the specimen. To restore breast shape, it could be necessary to mobilize breast tissue. Haemostasis needs to be done carefully.
Closure: Usually, the skin and subcutaneous tissue layers are closed together.
A secondary incision is typically made behind the lateral border of the pectoralis major in order to perform the axillary node biopsy, sample, and clearing. Patients whose axilla is not clinically involved can benefit from sentinal node biopsy. Before surgery, radioactive tracer is injected into the breast, then on the day of the procedure, blue dye (methylene blue) is injected. To facilitate histological examination, the initial draining nodes are located and excised. Usually, an axillary clearing is carried out if there are implicated nodes. The pectoralis minor is used to determine the levels of axillary clearance, with level 1 nodes up to the muscle, level II nodes behind it, and level III nodes beyond the subclavius. The axillary vessels, thoracodorsal nerve and vessels (supply latissimus dorsi), and the long thoracic nerve of Bell (to serratus anterior) should be carefully dissected. The intercostobrachial nerve, which passes laterally through the axilla, may need to be sacrificed. Usually, a drain is left in place after clearing.
Complications
bleeding, seroma, infection, and inadequate cosmesis. following axillary surgery: winged scapula (long thoracic nerve injury), frozen shoulder, discomfort, lymphoedema, and numbness (intercostobrachial nerve injury).
0 Comments
