- Published on
Surgery - Septic Arthritis
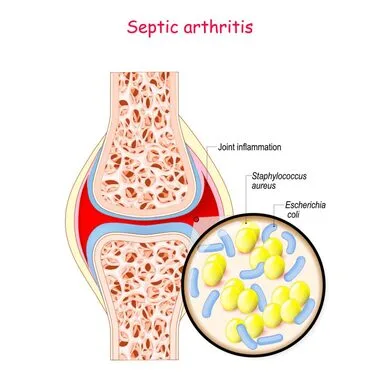
intra-articular joint infection.
Introduction
Bacteria can penetrate the joint directly, such as through a puncture wound, or they might spread hemorrhagically from nearby osteomyelitis or from a contaminated prosthesis. An inflammatory response in the joint is triggered by bacteria. A joint effusion is caused by permeability and fluid secretion. Activation of neutrophils and macrophages results in the production of proteolytic enzymes, which, in conjunction with bacterial toxins, cause destruction to the articular cartilage. Fibrosis and bony ankylosis may occur as a result of the raw articular surfaces recovering during the healing process.
Staphylococcus aureus, Neisseria gonorrhoeae in adults, and Haemophilus influenzae or coliforms are the most often occurring causal organisms in children under three years old.
R isk Factors
Septic arthritis is more common in those with diabetes, IV drug misuse, immunocompromised individuals, and those with chronic joint diseases (such as rheumatoid arthritis).
Epidemiology
50% of cases in children under three years old, incidence 6/100,000.
History
fever, malaise, and joint or limb pain.
usually only affects one big joint, such as the hip in young children, who may exhibit a limp and a refusal to bear weight. While it can affect any joint, older children and adults are more likely to have knee pain.
Examination
a red, swollen joint; if it's the hip, hold the leg flexed and move it slightly outside to loosen up the ligaments and lessen joint strain.
widespread joint soreness accompanied by a sharp decrease in range of motion.
Skin pustules in the vicinity of the joint may be present if gonococcal arthritis is present.
Investigations
Blood: CRP, ESR, FBC, and blood cultures.
Together with microscopy, culture, and sensitivity, aspiration Aspirate typically murky material including several neutrophils; culture to determine the causing pathogen.
Joint space, soft tissue edema, and in severe cases, subchondral bone loss are all seen on a joint radiograph.
Joint region shows increased absorption on a bone scan.
USS: May direct aspiration in order to detect a joint effusion.
Management
Surgical: To remove pus and infectious material, surgical washout of the joint is usually necessary. may be carried out through an open operation (arthrotomy) or by arthroscopy.
When a prosthetic joint develops sepsis, the prosthesis must be removed in order to completely eradicate the infection.
Health: IV antibiotics for two weeks at first, then oral antibiotics for a further four to six weeks.
For pain relief, analgesics and a splint should be applied to the joint.
To keep joints mobile and avoid fibrosis, physiotherapy is offered.
Complications
Joint damage or dislocation, growth disturbance, ankylosis, avascular necrosis of the epiphysis, or subsequent osteoarthritis.
Prognosis
Outcomes are depending on the virulence of the organism, duration of infection previous to diagnosis, the pre-morbid status of the patient and the joint affected; e.g. knees have better outcomes than ankles. The prognosis is often favorable with prompt, proper therapy.
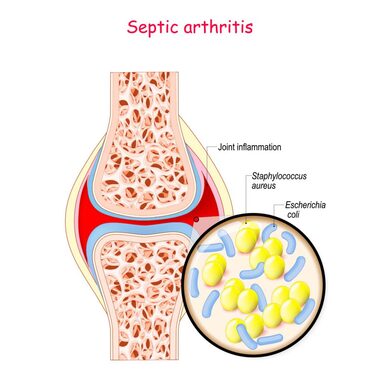
intra-articular joint infection.
Introduction
Bacteria can penetrate the joint directly, such as through a puncture wound, or they might spread hemorrhagically from nearby osteomyelitis or from a contaminated prosthesis. An inflammatory response in the joint is triggered by bacteria. A joint effusion is caused by permeability and fluid secretion. Activation of neutrophils and macrophages results in the production of proteolytic enzymes, which, in conjunction with bacterial toxins, cause destruction to the articular cartilage. Fibrosis and bony ankylosis may occur as a result of the raw articular surfaces recovering during the healing process.
Staphylococcus aureus, Neisseria gonorrhoeae in adults, and Haemophilus influenzae or coliforms are the most often occurring causal organisms in children under three years old.
R isk Factors
Septic arthritis is more common in those with diabetes, IV drug misuse, immunocompromised individuals, and those with chronic joint diseases (such as rheumatoid arthritis).
Epidemiology
50% of cases in children under three years old, incidence 6/100,000.
History
fever, malaise, and joint or limb pain.
usually only affects one big joint, such as the hip in young children, who may exhibit a limp and a refusal to bear weight. While it can affect any joint, older children and adults are more likely to have knee pain.
Examination
a red, swollen joint; if it's the hip, hold the leg flexed and move it slightly outside to loosen up the ligaments and lessen joint strain.
widespread joint soreness accompanied by a sharp decrease in range of motion.
Skin pustules in the vicinity of the joint may be present if gonococcal arthritis is present.
Investigations
Blood: CRP, ESR, FBC, and blood cultures.
Together with microscopy, culture, and sensitivity, aspiration Aspirate typically murky material including several neutrophils; culture to determine the causing pathogen.
Joint space, soft tissue edema, and in severe cases, subchondral bone loss are all seen on a joint radiograph.
Joint region shows increased absorption on a bone scan.
USS: May direct aspiration in order to detect a joint effusion.
Management
Surgical: To remove pus and infectious material, surgical washout of the joint is usually necessary. may be carried out through an open operation (arthrotomy) or by arthroscopy.
When a prosthetic joint develops sepsis, the prosthesis must be removed in order to completely eradicate the infection.
Health: IV antibiotics for two weeks at first, then oral antibiotics for a further four to six weeks.
For pain relief, analgesics and a splint should be applied to the joint.
To keep joints mobile and avoid fibrosis, physiotherapy is offered.
Complications
Joint damage or dislocation, growth disturbance, ankylosis, avascular necrosis of the epiphysis, or subsequent osteoarthritis.
Prognosis
Outcomes are depending on the virulence of the organism, duration of infection previous to diagnosis, the pre-morbid status of the patient and the joint affected; e.g. knees have better outcomes than ankles. The prognosis is often favorable with prompt, proper therapy.
0 Comments
