- Published on
Surgery - Stomas
Indications for Stomas
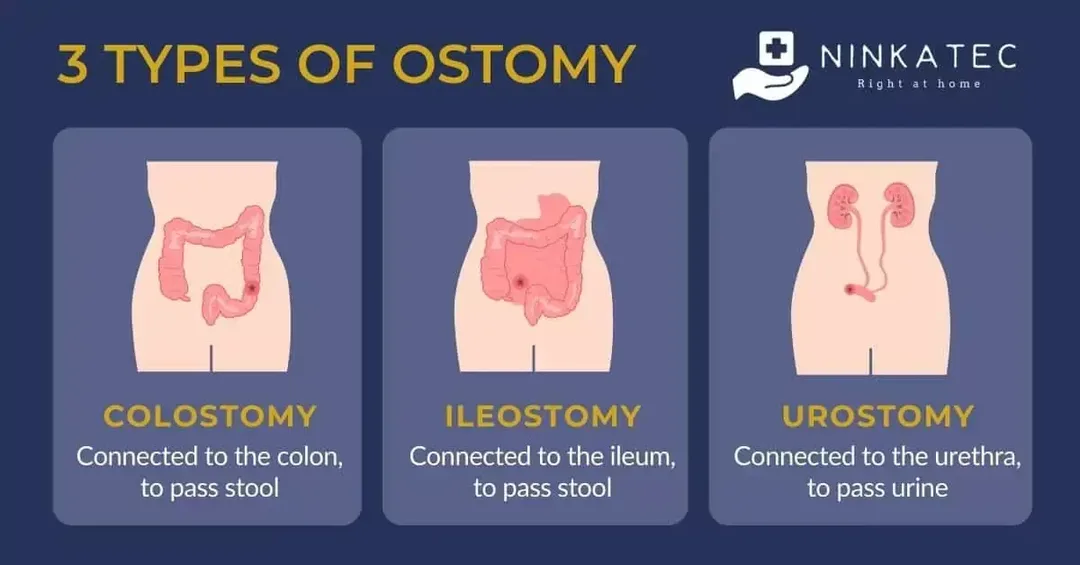
an incision made in surgery that connects the bladder or intestine to a bodily surface. Ileostomy, colostomy, and urostomy are the most common types of stomas; oesophagostomy, gastrostomy, jejunostomy, and caecostomy are among the others. End or loop stomas, either permanent or temporary. Malignancy in inflammatory bowel disease is optional. After a panproctocolectomy for familial polyposis or ulcerative colitis, stop ileostomies. following abdominoperineal excision for low rectal carcinomas, permanent colostomies. Loop stomas are used to temporarily divert bowel contents from sick sections of the intestines in order to safeguard distal surgery, such as an ileoanal pouch or low colorectal anastomosis, or to restore the anal sphincter.
Emergency: Ischemic bowel illness, inflammatory bowel damage, perforation, blockage, and toxic megacolon. During a Hartmann procedure, the distal end of the divided bowel is sealed or made into a mucous fistula, and the diseased distal colon is removed with the creation of an end colostomy.
Anatomy
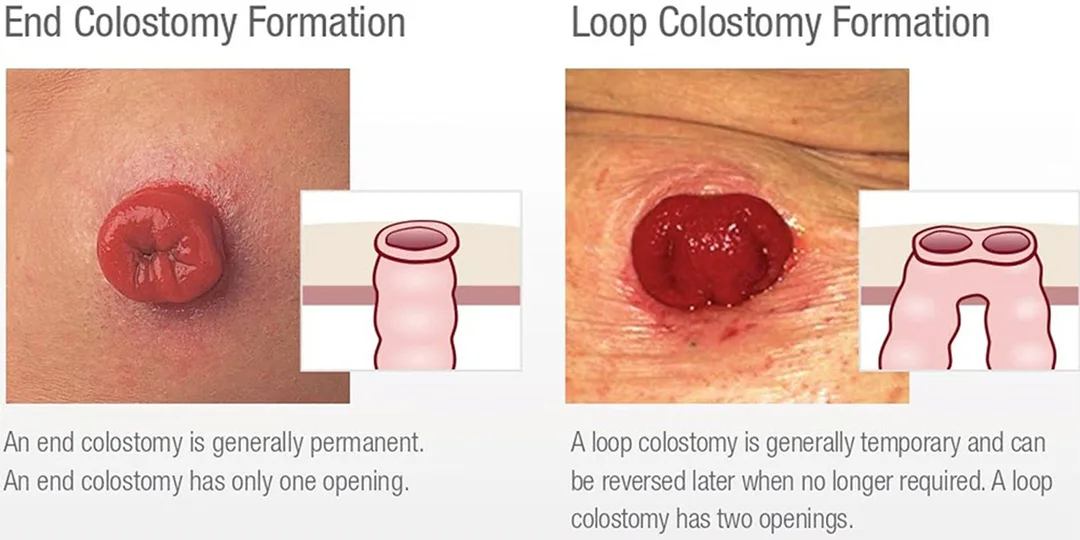
End stoma: To create the stoma, the colon is divided and its proximal end is brought through the abdominal wall. The distal end can form a double barrel stoma in the same opening, be closed and left in the belly, or be brought out through a different incision called a mucous fistula.
Loop stomas: A stoma with two lumens is created by raising a bowel loop to the surface, opening it, then folding it back on itself. may be simpler to shut. A certain amount of "spillover" of the nearest contents.
Ileostomies: Located in the right iliac fossa, albeit not necessarily. They are designed with a spout that protrudes 2.5 cm above the skin's surface because the discharge is irritating. Liquid output occurs at a rate of 1-2 L per day, however it may decrease after a few weeks.
Colostomies: The stoma is flush with the skin and is typically located in the LIF, though it can be anywhere. Depending on the diet, the output is sporadic and has a more solid consistency (although transverse colostomies can produce semi-liquid, which can be more challenging to control).
Appliances for stomas: Comprised of a flange, which covers and shields the skin surrounding the stoma, and a pouch. There could be one or two pieces in the flange; when the pouch is changed, the second component stays affixed to the skin for a few days. Additionally, some bags feature exit drains for liquid outflow (ileostomies, for example). The smell of flatus can be lessened by using charcoal filters.
Investigations
Pre-op: Stoma placement and counseling are crucial, however they aren't always feasible in emergency cases. Specialist nurses in stoma care are essential. Pre-operative stomas should be identified so the patient can see it; skinfolds, scars, bony prominences, and the belt line should all be avoided. You might need to prepare your intestines. It is frequently necessary to have distal contrast investigations before stoma reversal. Prophylactic DVT after surgery. Support and education for patients in managing their stomas.
Procedure
Skin incision: A circular skin incision is made at the designated stoma site (using the rectus muscle to place a stoma reduces the risk of parastomal hernia development). A cut is made in the skin, the fascia is separated, the muscle is split, and the peritoneum is opened (to allow room for two fingers).
Formation of a stoma: The bowel's loop or end is brought out through the aperture. This gut should be well-vascularized, stress-free, and trauma-free. The primary incision has been treated and sealed. If the bowel is a loop or has been stapled in the past, it is opened, and the edges are cleansed. The bowel is turned inside out and the skin is sutured around the margins. Next, a transparent stoma bag is placed to enable routine stoma examination.
Complications
40% for ileostomies and 20% for colostomies, with 15% requiring surgical repair, are relatively common.
Death: becomes apparent a few hours after surgery and necessitates stoma modification because it compromises the bowel's blood flow during stoma development.
Haemorrhage: In most cases, only little bleeding needs medical attention. Practical: either constipation or diarrhea. Large volume liquid output from ileostomies can cause electrolyte imbalances and dehydration, which can be treated with fluid replacement and prescription drugs like codeine and loperamide. Hydration is crucial because urinary tract calculi are more likely in those who have an ileostomy.
Additional conditions include skin irritation, leaks, prolapses or retractions that occasionally need to be refashioned, stenosis (which can sometimes be widened using a dilator), parastomal hernias, abscesses, or fistulas.
Psychological: Anxiety, shame, or issues with body image.
Indications for Stomas
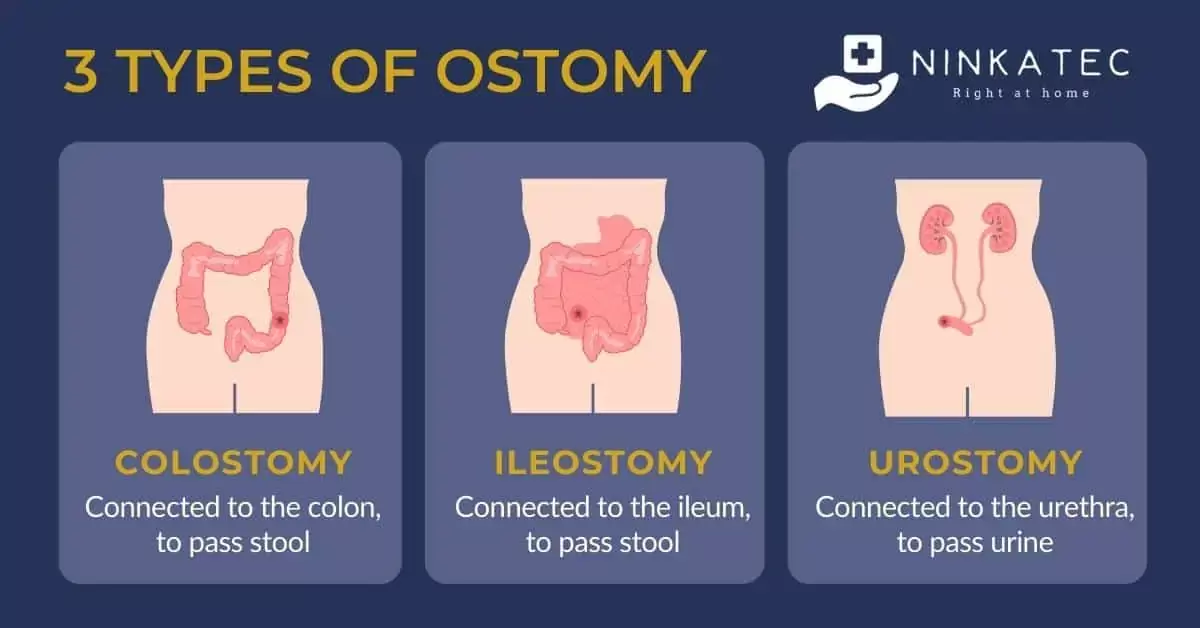
an incision made in surgery that connects the bladder or intestine to a bodily surface. Ileostomy, colostomy, and urostomy are the most common types of stomas; oesophagostomy, gastrostomy, jejunostomy, and caecostomy are among the others. End or loop stomas, either permanent or temporary. Malignancy in inflammatory bowel disease is optional. After a panproctocolectomy for familial polyposis or ulcerative colitis, stop ileostomies. following abdominoperineal excision for low rectal carcinomas, permanent colostomies. Loop stomas are used to temporarily divert bowel contents from sick sections of the intestines in order to safeguard distal surgery, such as an ileoanal pouch or low colorectal anastomosis, or to restore the anal sphincter.
Emergency: Ischemic bowel illness, inflammatory bowel damage, perforation, blockage, and toxic megacolon. During a Hartmann procedure, the distal end of the divided bowel is sealed or made into a mucous fistula, and the diseased distal colon is removed with the creation of an end colostomy.
Anatomy
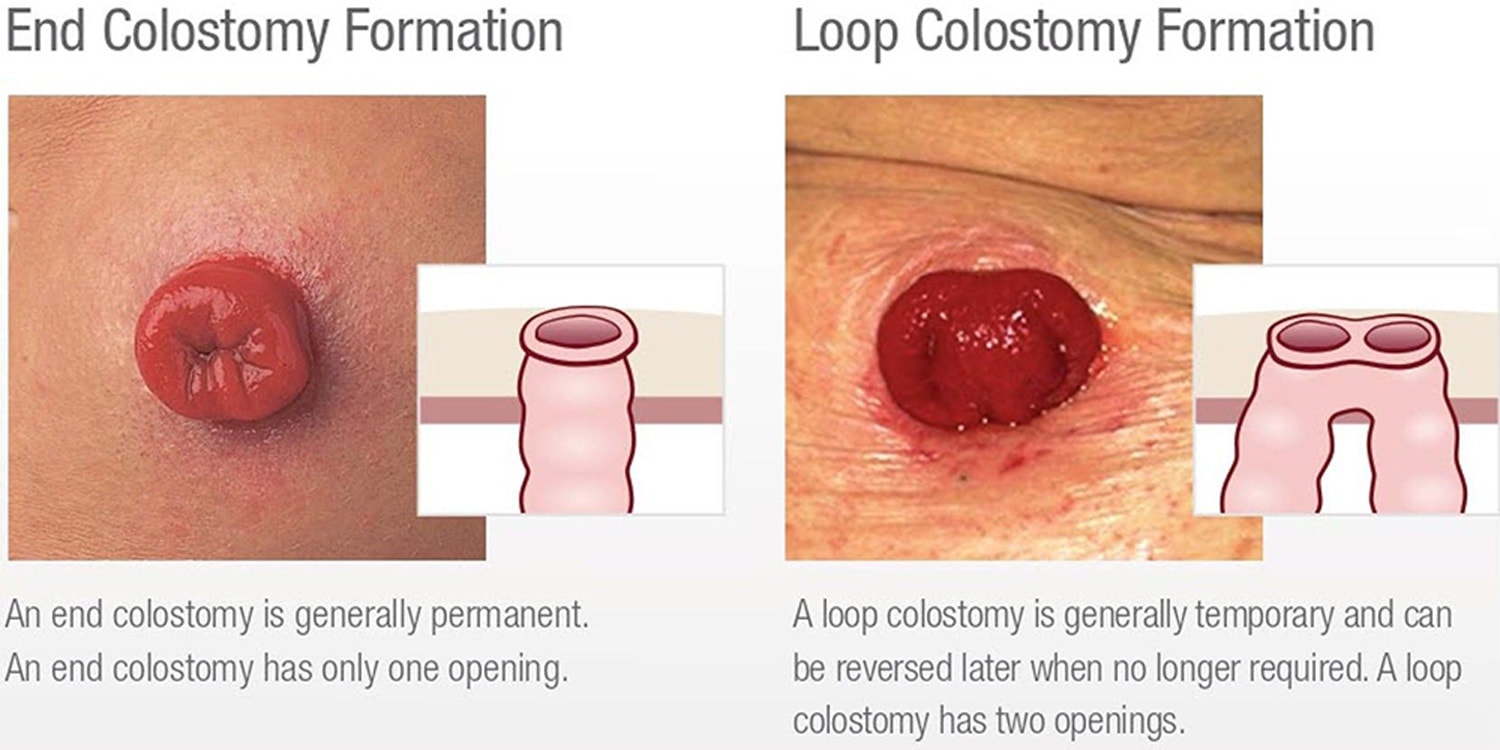
End stoma: To create the stoma, the colon is divided and its proximal end is brought through the abdominal wall. The distal end can form a double barrel stoma in the same opening, be closed and left in the belly, or be brought out through a different incision called a mucous fistula.
Loop stomas: A stoma with two lumens is created by raising a bowel loop to the surface, opening it, then folding it back on itself. may be simpler to shut. A certain amount of "spillover" of the nearest contents.
Ileostomies: Located in the right iliac fossa, albeit not necessarily. They are designed with a spout that protrudes 2.5 cm above the skin's surface because the discharge is irritating. Liquid output occurs at a rate of 1-2 L per day, however it may decrease after a few weeks.
Colostomies: The stoma is flush with the skin and is typically located in the LIF, though it can be anywhere. Depending on the diet, the output is sporadic and has a more solid consistency (although transverse colostomies can produce semi-liquid, which can be more challenging to control).
Appliances for stomas: Comprised of a flange, which covers and shields the skin surrounding the stoma, and a pouch. There could be one or two pieces in the flange; when the pouch is changed, the second component stays affixed to the skin for a few days. Additionally, some bags feature exit drains for liquid outflow (ileostomies, for example). The smell of flatus can be lessened by using charcoal filters.
Investigations
Pre-op: Stoma placement and counseling are crucial, however they aren't always feasible in emergency cases. Specialist nurses in stoma care are essential. Pre-operative stomas should be identified so the patient can see it; skinfolds, scars, bony prominences, and the belt line should all be avoided. You might need to prepare your intestines. It is frequently necessary to have distal contrast investigations before stoma reversal. Prophylactic DVT after surgery. Support and education for patients in managing their stomas.
Procedure
Skin incision: A circular skin incision is made at the designated stoma site (using the rectus muscle to place a stoma reduces the risk of parastomal hernia development). A cut is made in the skin, the fascia is separated, the muscle is split, and the peritoneum is opened (to allow room for two fingers).
Formation of a stoma: The bowel's loop or end is brought out through the aperture. This gut should be well-vascularized, stress-free, and trauma-free. The primary incision has been treated and sealed. If the bowel is a loop or has been stapled in the past, it is opened, and the edges are cleansed. The bowel is turned inside out and the skin is sutured around the margins. Next, a transparent stoma bag is placed to enable routine stoma examination.
Complications
40% for ileostomies and 20% for colostomies, with 15% requiring surgical repair, are relatively common.
Death: becomes apparent a few hours after surgery and necessitates stoma modification because it compromises the bowel's blood flow during stoma development.
Haemorrhage: In most cases, only little bleeding needs medical attention. Practical: either constipation or diarrhea. Large volume liquid output from ileostomies can cause electrolyte imbalances and dehydration, which can be treated with fluid replacement and prescription drugs like codeine and loperamide. Hydration is crucial because urinary tract calculi are more likely in those who have an ileostomy.
Additional conditions include skin irritation, leaks, prolapses or retractions that occasionally need to be refashioned, stenosis (which can sometimes be widened using a dilator), parastomal hernias, abscesses, or fistulas.
Psychological: Anxiety, shame, or issues with body image.
0 Comments
