- Published on
Surgery - Subarachnoid Hemorrhage
Introduction
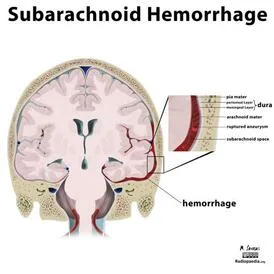
Bleed into the subarachnoid space, which is the area between the pia mater, which protects the brain and spinal cord, and the arachnoid mater, which lines the interior side of the dura. This space contains CSF.
Etiology
85% rupture of a saccular aneurysm (berry aneurysm), 5% AVMs.
Additional reasons include mycotic aneurysms, trauma, perimesencephalic hemorrhage, and drug addiction (e.g., cocaine).
Epidemiology
The yearly occurrence of 10/100,000. maximum age in the 1950s.
History
An acute, intense headache that is traditionally described as feeling like a "hit to the back of the head."
Associated symptoms include photophobia, neck stiffness, and nausea.
Perplexity, breakdown, or # awareness level.
Examination
Meningism is characterized by stiff neck and Kernig's sign, which is pain or resistance to knee extension when the hip is flexed and is caused by blood irritating the meninges.
Glasgow Coma Rating System: Evaluate and periodically check for decline.
Three components make up the Glasgow Coma Scale (GCS); the lowest score is 3 and the highest score is 15.
Papilloedema and IVth or IIIrd cranial nerve palsy (the latter may potentially be caused by pressure from a posterior communicating artery aneurysm) are indications of elevated intracranial pressure.
Subhyaloid hemorrhage between the vitreous membrane and retina was discovered by fundoscopy.
Focal neurological signs: Usually brought on by diminished brain perfusion and ischemia from vasospasm.
Pathogenesis
abnormal localized blood artery dilatation, typically observed at the locations where the arteries split in the Willis circle, where a congenital or acquired vessel wall weakening is thought to exist. Saccular aneurysms are linked to Ehlers-Danlos syndrome, Marfan's syndrome, pseudoxanthoma elasticum, and polycystic kidney disease. Twenty percent of people have several aneurysms.
Investigations
Blood: coagulation, G&S, ESR, CRP, U&Es, and FBC.
On a CT scan, hyperdense patches in the subarachnoid space—typically in the Sylvian fissure or basal chambers—represent blood. There might be hydrocephalus present as well.
Angiography (MRI, CT, or intra-arterial four-vessel): To identify the bleeding location in patients who may benefit from endovascular or surgical procedures.
Lumbar puncture: spectrophotometry of the CSF supernatant following centrifugation revealed the following: "Opening pressure," "RBC," low WCC, and xanthochromia (straw-colored CSF) caused by breakdown of Hb.
Management
Acute: Maintain bed rest, analgesics (codeine or paracetamol), IV fluids to maintain cerebral perfusion (use 0.9% saline; avoid sucrose as it may exacerbate hyponatraemia and increased cerebral oedema), and seek prompt neurosurgical assessment. To avoid vasospasm, imidipine should be used every four hours.
Interventional neuroradiology: Aneurysm coiling, typically with platinum. According to the ISAT experiment, the results are comparable to neurosurgery, if not better.
Surgical: If neuroradiological intervention is not effective for aneurysm, then the aneurysm may need to be clipped or wrapped.
Complications
25 percent of cases of hydrocephalus are caused by blood impeding CSF flow or resorption through arachnoid villi.
cerebral vasospasm, which appears 2-4 days following a hemorrhage.
Hyponatraemia (perhaps brought on by cerebral salt-wasting disease or SIADH).
severe neurological impairments based on the bleeding place.
Prognosis
high death rate (over 30% in the initial days). A lower GCS or a neurological abnormality upon presentation are associated with a worse prognosis. During the first two months without treatment, there is a significant chance of a serious rebleed. reduced death rate compared to aneurysmal bleeds in situations of perimesencephalic subarachnoid hemorrhage.
Introduction
Bleed into the subarachnoid space, which is the area between the pia mater, which protects the brain and spinal cord, and the arachnoid mater, which lines the interior side of the dura. This space contains CSF.
Etiology
85% rupture of a saccular aneurysm (berry aneurysm), 5% AVMs.
Additional reasons include mycotic aneurysms, trauma, perimesencephalic hemorrhage, and drug addiction (e.g., cocaine).
Epidemiology
The yearly occurrence of 10/100,000. maximum age in the 1950s.
History
An acute, intense headache that is traditionally described as feeling like a "hit to the back of the head."
Associated symptoms include photophobia, neck stiffness, and nausea.
Perplexity, breakdown, or # awareness level.
Examination
Meningism is characterized by stiff neck and Kernig's sign, which is pain or resistance to knee extension when the hip is flexed and is caused by blood irritating the meninges.
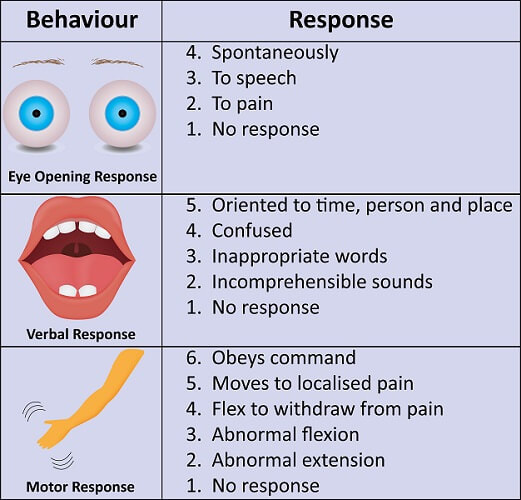
Glasgow Coma Rating System: Evaluate and periodically check for decline.
Three components make up the Glasgow Coma Scale (GCS); the lowest score is 3 and the highest score is 15.
Papilloedema and IVth or IIIrd cranial nerve palsy (the latter may potentially be caused by pressure from a posterior communicating artery aneurysm) are indications of elevated intracranial pressure.
Subhyaloid hemorrhage between the vitreous membrane and retina was discovered by fundoscopy.
Focal neurological signs: Usually brought on by diminished brain perfusion and ischemia from vasospasm.
Pathogenesis
abnormal localized blood artery dilatation, typically observed at the locations where the arteries split in the Willis circle, where a congenital or acquired vessel wall weakening is thought to exist. Saccular aneurysms are linked to Ehlers-Danlos syndrome, Marfan's syndrome, pseudoxanthoma elasticum, and polycystic kidney disease. Twenty percent of people have several aneurysms.
Investigations
Blood: coagulation, G&S, ESR, CRP, U&Es, and FBC.
On a CT scan, hyperdense patches in the subarachnoid space—typically in the Sylvian fissure or basal chambers—represent blood. There might be hydrocephalus present as well.
Angiography (MRI, CT, or intra-arterial four-vessel): To identify the bleeding location in patients who may benefit from endovascular or surgical procedures.
Lumbar puncture: spectrophotometry of the CSF supernatant following centrifugation revealed the following: "Opening pressure," "RBC," low WCC, and xanthochromia (straw-colored CSF) caused by breakdown of Hb.
Management
Acute: Maintain bed rest, analgesics (codeine or paracetamol), IV fluids to maintain cerebral perfusion (use 0.9% saline; avoid sucrose as it may exacerbate hyponatraemia and increased cerebral oedema), and seek prompt neurosurgical assessment. To avoid vasospasm, imidipine should be used every four hours.
Interventional neuroradiology: Aneurysm coiling, typically with platinum. According to the ISAT experiment, the results are comparable to neurosurgery, if not better.
Surgical: If neuroradiological intervention is not effective for aneurysm, then the aneurysm may need to be clipped or wrapped.
Complications
25 percent of cases of hydrocephalus are caused by blood impeding CSF flow or resorption through arachnoid villi.
cerebral vasospasm, which appears 2-4 days following a hemorrhage.
Hyponatraemia (perhaps brought on by cerebral salt-wasting disease or SIADH).
severe neurological impairments based on the bleeding place.
Prognosis
high death rate (over 30% in the initial days). A lower GCS or a neurological abnormality upon presentation are associated with a worse prognosis. During the first two months without treatment, there is a significant chance of a serious rebleed. reduced death rate compared to aneurysmal bleeds in situations of perimesencephalic subarachnoid hemorrhage.
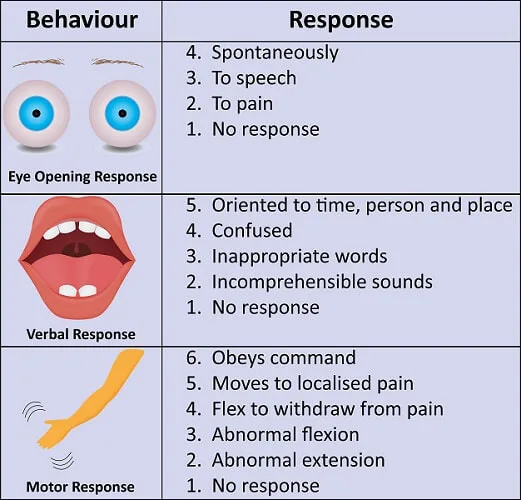
Glasgow Coma Scale
0 Comments
