- Published on
Surgery - Subdural Hemorrhage
Introduction
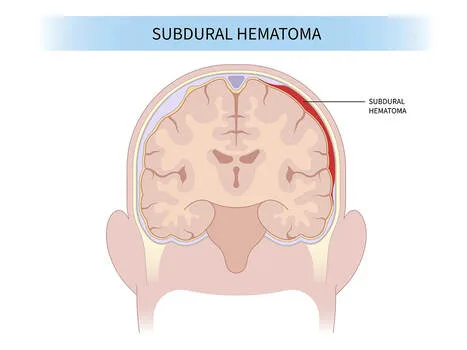
A collection of blood that forms between the dura mater and the brain's surface is known as a subdural haematoma (SDH).
Acute: In less than a week.
Subacute: 18 to 24 hours.
Chronic: Three weeks in.
Etiology
Shearing pressures from trauma that causes the brain to accelerate and decelerate quickly rip the "bridging veins," or veins that connect the dura to the cortex. Between the dura and arachnoid membranes, bleeding takes place.
Non-accidental injury in children should always be taken into account.
Epidemiology
Acute: Usually affects younger individuals and is linked to significant trauma (5–25% of cases of severe head injuries). greater in frequency than extradural hemorrhage.
Chronic: Research indicates that the incidence of this condition is 1-2/5/100,000 in the elderly.
History
Acute: Patient has a history of head trauma and is not fully aware.
Subacute: Changing mental status and increasing headaches 7–14 days after injury.
Chronic: May show up as focal weakness, headache, disorientation, cognitive decline, mental symptoms, or seizures.
Have a low index of suspicion, especially in the case of older people and alcoholics, as there may not be a history of trauma or falls.
Examination
Acute: Lower GCS. Large hemorrhages that cause a midline shift can also cause bradycardia, diminished consciousness, and an ipsilateral fixed dilated pupil due to compression of the ipsilateral IIIrd nerve parasympathetic fibres.
Chronic: There may be focal neurological signs (hemiparesis, reflex asymmetry, papilloedema, malfunction of the IIIrd or VIth nerves), but neurological testing may be normal.
Investigations
The CT head is a lump with a crescent or sickle shape that is concave across the surface of the brain (an extradural has a lentiform shape). The CT look varies over time. Chronic subdurals are hypodense (approaching that of CSF) while acute subdurals are hyperdense (becoming isodense over 1-3 weeks; presence may be inferred from indications such as effacement of sulci, midline shift, ventricular compression, and obliteration of basal cisterns).
The brain's MRI is more sensitive, particularly for isodense or tiny SDHs.
Management
Acute: ABC and cervical spine control are given priority in the ATLS procedure. Cervical spine injuries are far more likely to occur following a head injury. GCS and pupillary reactivity are disabilities. Lift your head and think about osmotic diuresis with mannitol and/or hyperventilation if there are indications of an elevated ICP. After stabilization, take the CT head.
Cautious: Particularly when there is a tiny and minor midline shift (SDH <10 mm in thickness and <5 mm in midline shift).
Surgical: For symptomatic subdurals larger than 10 mm, promptly do a burr hole or craniotomy and evacuation, with a midline displacement of more than 5 mm (best if within 4 hours). Devices for ICP monitoring could be installed.
Chronic: Surgical treatment with a burr hole or craniotomy and drainage (a drain may be left in for 24–72 hours) if there is symptomatic or a mass effect on imaging. The recommended course of treatment for asymptomatic SDH without a noticeable mass effect is to use serial imaging to watch for spontaneous resorption. Resorbing hematomas can necessitate a craniotomy along with a membranectomy.
Younger children: If open fontanelle percutaneous aspiration is not successful, a subdural to peritoneal shunt can be implanted.
Complications
Increased intracranial pressure, cerebral edema that may lead to further ischemic brain injury, and mass effect (such as a transtentorial or uncal herniation).
After surgery: The following conditions are relatively common: intracerebral hemorrhage, subdural empyema, meningitis or brain abscess, tension pneumocephalus, seizures, and recurrence (up to 33% for SDH).
Prognosis
Acute: The primary determinant of outcome is the underlying brain damage.
Because there is a lower frequency of underlying brain injury, chronic SDHs often have better results than acute SDHs; three-fourths of patients treated with surgery have satisfactory outcomes.
Introduction
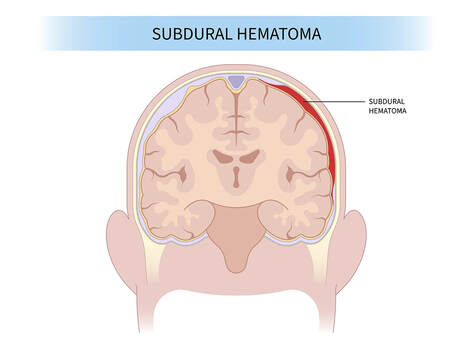
A collection of blood that forms between the dura mater and the brain's surface is known as a subdural haematoma (SDH).
Acute: In less than a week.
Subacute: 18 to 24 hours.
Chronic: Three weeks in.
Etiology
Shearing pressures from trauma that causes the brain to accelerate and decelerate quickly rip the "bridging veins," or veins that connect the dura to the cortex. Between the dura and arachnoid membranes, bleeding takes place.
Non-accidental injury in children should always be taken into account.
Epidemiology
Acute: Usually affects younger individuals and is linked to significant trauma (5–25% of cases of severe head injuries). greater in frequency than extradural hemorrhage.
Chronic: Research indicates that the incidence of this condition is 1-2/5/100,000 in the elderly.
History
Acute: Patient has a history of head trauma and is not fully aware.
Subacute: Changing mental status and increasing headaches 7–14 days after injury.
Chronic: May show up as focal weakness, headache, disorientation, cognitive decline, mental symptoms, or seizures.
Have a low index of suspicion, especially in the case of older people and alcoholics, as there may not be a history of trauma or falls.
Examination
Acute: Lower GCS. Large hemorrhages that cause a midline shift can also cause bradycardia, diminished consciousness, and an ipsilateral fixed dilated pupil due to compression of the ipsilateral IIIrd nerve parasympathetic fibres.
Chronic: There may be focal neurological signs (hemiparesis, reflex asymmetry, papilloedema, malfunction of the IIIrd or VIth nerves), but neurological testing may be normal.
Investigations
The CT head is a lump with a crescent or sickle shape that is concave across the surface of the brain (an extradural has a lentiform shape). The CT look varies over time. Chronic subdurals are hypodense (approaching that of CSF) while acute subdurals are hyperdense (becoming isodense over 1-3 weeks; presence may be inferred from indications such as effacement of sulci, midline shift, ventricular compression, and obliteration of basal cisterns).
The brain's MRI is more sensitive, particularly for isodense or tiny SDHs.
Management
Acute: ABC and cervical spine control are given priority in the ATLS procedure. Cervical spine injuries are far more likely to occur following a head injury. GCS and pupillary reactivity are disabilities. Lift your head and think about osmotic diuresis with mannitol and/or hyperventilation if there are indications of an elevated ICP. After stabilization, take the CT head.
Cautious: Particularly when there is a tiny and minor midline shift (SDH <10 mm in thickness and <5 mm in midline shift).
Surgical: For symptomatic subdurals larger than 10 mm, promptly do a burr hole or craniotomy and evacuation, with a midline displacement of more than 5 mm (best if within 4 hours). Devices for ICP monitoring could be installed.
Chronic: Surgical treatment with a burr hole or craniotomy and drainage (a drain may be left in for 24–72 hours) if there is symptomatic or a mass effect on imaging. The recommended course of treatment for asymptomatic SDH without a noticeable mass effect is to use serial imaging to watch for spontaneous resorption. Resorbing hematomas can necessitate a craniotomy along with a membranectomy.
Younger children: If open fontanelle percutaneous aspiration is not successful, a subdural to peritoneal shunt can be implanted.
Complications
Increased intracranial pressure, cerebral edema that may lead to further ischemic brain injury, and mass effect (such as a transtentorial or uncal herniation).
After surgery: The following conditions are relatively common: intracerebral hemorrhage, subdural empyema, meningitis or brain abscess, tension pneumocephalus, seizures, and recurrence (up to 33% for SDH).
Prognosis
Acute: The primary determinant of outcome is the underlying brain damage.
Because there is a lower frequency of underlying brain injury, chronic SDHs often have better results than acute SDHs; three-fourths of patients treated with surgery have satisfactory outcomes.
0 Comments
