- Published on
Surgery - Testicular Torsion
Definition
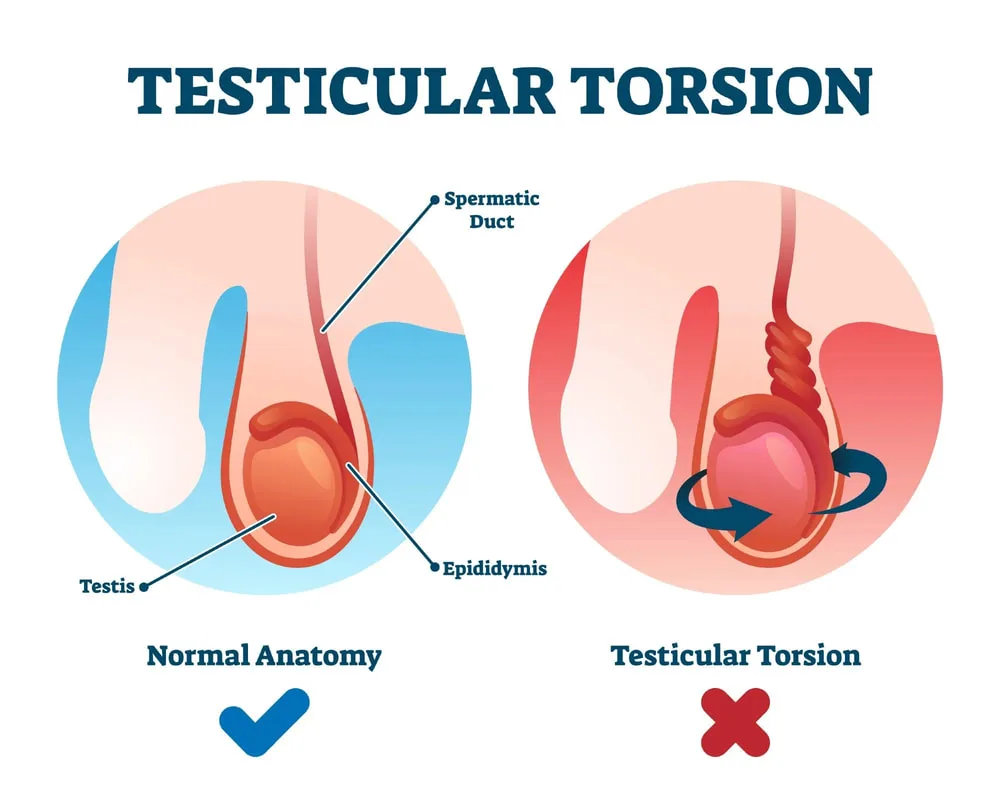
An urgent surgical procedure is required to treat spermatic cord twisting or torsion, which first obstructs the testis's venous outflow and, if left untreated, progresses to artery occlusion and testicular infarction.
Etiology
Intravaginal (most common type): The testis might twist inside the vaginalis due to a large investment of the tunica vaginalis around the spermatic cord.
Extravaginal (found in newborns): A condition in which the spermatic cord twists along a vertical axis, causing the entire testes and tunica vaginalis to twist (since the gubernaculum is not fully fixed to the scrotal wall, allowing for unrestricted rotation).
Risk Factors
Bell clapper testes, or imperfectly descending testes, have a large investment in the tunica vaginalis, and the epididymal mesentery is lengthy.
Epidemiology
Incidence each year: 1 in 4000. The most frequent cause of acute scrotal pain in children aged 10 to 18 is intravaginal. exceptionally uncommon in newborns (extravaginal torsion).
H HISTORY
strong hemiscrotal pain that develops suddenly and may be accompanied by nausea, vomiting, and stomach pain. The patient may have discomfort upon awakening from sleep or may have previously experienced a similar pain that resolved on its own.
Examination
The affected side may have an erythematous, swollen scrotum, a palpably thicker cord, and an anteriorly positioned epididymis. The testis may be extremely tender, positioned higher than the contralateral side, and horizontal. There might not be a cremasteric response.
Differential diagnosis: Appendix testes, appendix epididymis, and hydatid of Morgagni are examples of testicular appendix torsion. A lesion that is apparent via transillumination (blue dot sign) might exist.
Epididymo-orchitis with inguinal hernia in prison.
Pathogenesis
If the blood supply is not restored by detorsion, twisting causes compression of the veins of the pampiniform plexus from the testis and venous congestion, which leads to progressive ischaemia and infarction.
Investigational studies
Until proven otherwise, a young boy or adolescent with a very sensitive and swollen testis should be treated as if they have torsion, necessitating immediate investigation.
Testicular Doppler or Duplex Imaging: Surgery shouldn't be postponed, but it may be done.
In cases of torsion, arterial inflow may be decreased; in cases of epididymo-orchitis, it may cease.
Management
Surgical: Scrotal exploration should ideally be done within six hours of the onset of symptoms.
Counseling on bilateral orchidopexy and orchidectomy should be a part of consent. A transverse or midline raphe incision is done through the muscle of the dartos. The testis is delivered and examined after the tunica vaginalis is opened. The testis is untwisted, allowed to reperfuse, and then covered for a short while with a warm swab soaked in saline.
Bilateral orchidopexy is performed next. In order to stop recurrence, the testis was traditionally fixed in three places to the scrotal tissues using nonabsorbable sutures. An orchidectomy is carried out if it is discovered that the testis is necrotic.
Complications
Atrophy and infarction of the testicles if treatment is delayed. If left untreated, the testes could become infected or worsen fertility by encouraging the production of antibodies against sperm.
hemorrhage and infection following surgery.
Prognosis
A testicular torsion may only last 4-6 hours from the time pain starts.Most instances can be saved with quick investigation.
Definition
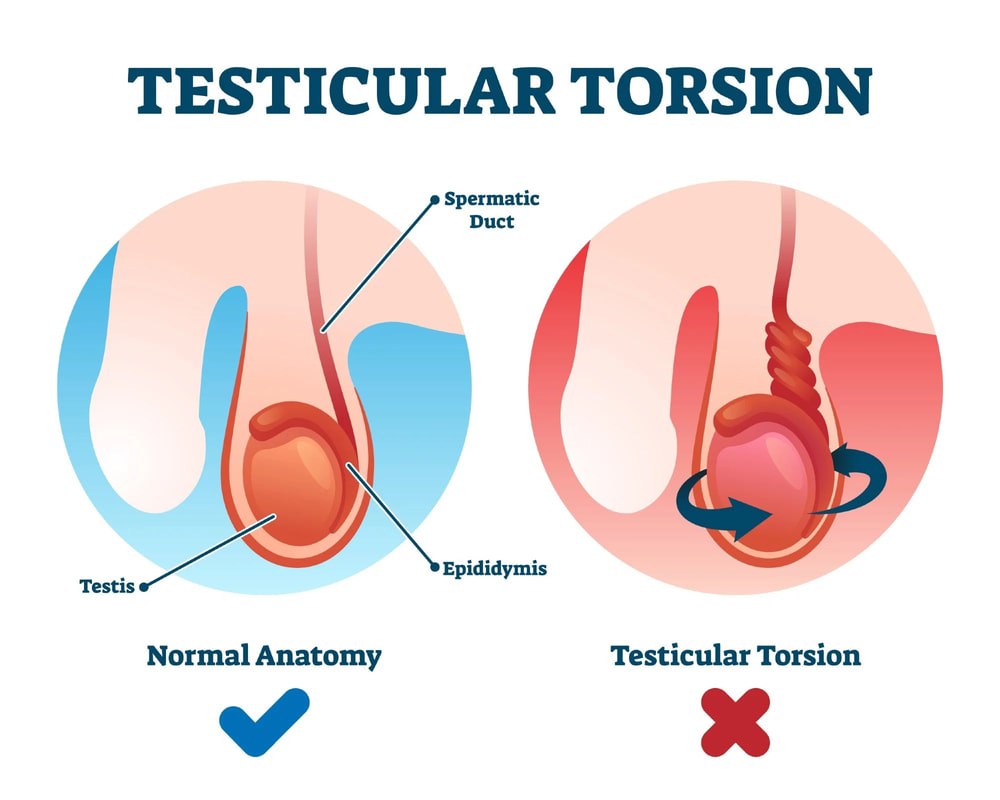
An urgent surgical procedure is required to treat spermatic cord twisting or torsion, which first obstructs the testis's venous outflow and, if left untreated, progresses to artery occlusion and testicular infarction.
Etiology
Intravaginal (most common type): The testis might twist inside the vaginalis due to a large investment of the tunica vaginalis around the spermatic cord.
Extravaginal (found in newborns): A condition in which the spermatic cord twists along a vertical axis, causing the entire testes and tunica vaginalis to twist (since the gubernaculum is not fully fixed to the scrotal wall, allowing for unrestricted rotation).
Risk Factors
Bell clapper testes, or imperfectly descending testes, have a large investment in the tunica vaginalis, and the epididymal mesentery is lengthy.
Epidemiology
Incidence each year: 1 in 4000. The most frequent cause of acute scrotal pain in children aged 10 to 18 is intravaginal. exceptionally uncommon in newborns (extravaginal torsion).
H HISTORY
strong hemiscrotal pain that develops suddenly and may be accompanied by nausea, vomiting, and stomach pain. The patient may have discomfort upon awakening from sleep or may have previously experienced a similar pain that resolved on its own.
Examination
The affected side may have an erythematous, swollen scrotum, a palpably thicker cord, and an anteriorly positioned epididymis. The testis may be extremely tender, positioned higher than the contralateral side, and horizontal. There might not be a cremasteric response.
Differential diagnosis: Appendix testes, appendix epididymis, and hydatid of Morgagni are examples of testicular appendix torsion. A lesion that is apparent via transillumination (blue dot sign) might exist.
Epididymo-orchitis with inguinal hernia in prison.
Pathogenesis
If the blood supply is not restored by detorsion, twisting causes compression of the veins of the pampiniform plexus from the testis and venous congestion, which leads to progressive ischaemia and infarction.
Investigational studies
Until proven otherwise, a young boy or adolescent with a very sensitive and swollen testis should be treated as if they have torsion, necessitating immediate investigation.
Testicular Doppler or Duplex Imaging: Surgery shouldn't be postponed, but it may be done.
In cases of torsion, arterial inflow may be decreased; in cases of epididymo-orchitis, it may cease.
Management
Surgical: Scrotal exploration should ideally be done within six hours of the onset of symptoms.
Counseling on bilateral orchidopexy and orchidectomy should be a part of consent. A transverse or midline raphe incision is done through the muscle of the dartos. The testis is delivered and examined after the tunica vaginalis is opened. The testis is untwisted, allowed to reperfuse, and then covered for a short while with a warm swab soaked in saline.
Bilateral orchidopexy is performed next. In order to stop recurrence, the testis was traditionally fixed in three places to the scrotal tissues using nonabsorbable sutures. An orchidectomy is carried out if it is discovered that the testis is necrotic.
Complications
Atrophy and infarction of the testicles if treatment is delayed. If left untreated, the testes could become infected or worsen fertility by encouraging the production of antibodies against sperm.
hemorrhage and infection following surgery.
Prognosis
A testicular torsion may only last 4-6 hours from the time pain starts.Most instances can be saved with quick investigation.
0 Comments
