- Published on
Surgery - Vascular Access
Indications
Obtaining access for dialysis: involves the formation of a fistula two to three months prior to the start of dialysis. A native fistula should ideally be created as far away as feasible to minimize the risk of heart strain and "steal syndrome" while simultaneously providing the ideal length for venous cannulation and allowing for the eventual construction of more proximal access if necessary.
Signs of a leg fistula include: Occlusion of the innominate vein or superior vena cava (usually as a result of prior central vein lines).
Severe obesity, central venous blockage, or exhausted peripheral veins are indications for transplant fistulas.
Central vein catheters: Necessary in cases of severe heart failure, peripheral vascular disease, or emergency hemodialysate without a functional fistula.
Anatomy
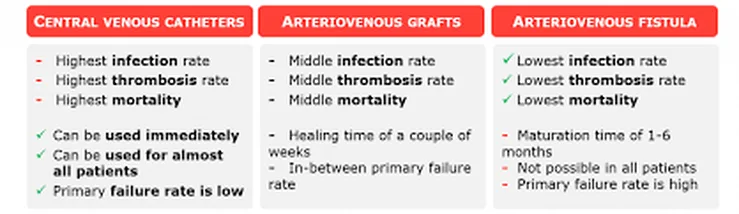
There are three primary methods available: central venous catheter, prosthetic arteriovenous graft, or native arteriovenous fistula (AVF).
Native fistulas: Brachiobasilic, brachiocephalic, atypical (ulnarbasilic or radiobasilic), more proximal radiocephalic (Brescia–Cimino), brachiocephalic, and upper leg (saphenous vein loop, saphenous vein in situ, and femoral vein loop).
Axillary artery to contralateral axillary vein (necklace graft), axillary loop graft, and contralateral IJV bypass graft are examples of complex vascular access operations. SFV transposition (SVC obstruction), femoro-femoral crossover bypass, and axillary artery-popliteal vein bypass graft (SVC obstruction in individuals with diabetes or obesity).
Catheters for the central vein: Single and dual lumen catheters, non-tunnelled (short-term) or tunnelled (cuffed to prevent infection).
Investigations
Thorough clinical evaluation of the venous and arterial anatomy prior to surgery. Allen examination. If necessary—for example, due to a history of vascular issues or assessment difficulties—duplex scanning can be used to evaluate vein patency, artery input, and caliber. Venogram in case the patency of the veins is in doubt.
Post-operative: Fistula assessment and clinical examination of bruit and thrill. Before native fistulae can be utilized for dialysis, they often need a few weeks to grow. One can needle grafts more rapidly.
Aftercare: measurement of the ultrasound dilution to gauge the cardiac output, recirculation rate, and graft input rate. A fistulogram and the required intervention, such as endovascular or surgical fistuloplasty of stenosis, can be carried out if the inflow is less than 600 ml/min, there has been a decline since the last evaluation, or the recirculation rate is greater than 5%.
Anaesthesia: Depending on the procedure, either a local, regional, or global block is used.
Procedure
The vein is evaluated, dissected, mobilized, and separated distally after the proper incision. After the artery is dissected and heparin is injected intravenously, it is clamped, and an arteriotomy is made. Prolene suture is used to perform a side-to-side anastomosis. For simple cannulation in brachiobasilic fistulae, the vein must be transferred into superficial subcutaneous tissue. The most common grafts utilized are looped, straight, or PTFE.
Catheters for the central vein: Internal jugular veins are typically utilized for placement under ultrasound guidance; femoral veins can be used, but only temporarily, because of the danger of thrombosis and infection.
Complications
Thrombosis, failure to mature, limb edema, aneurysmal dilatation, bleeding, infection, nerve injury, distal embolization, steal syndrome, and thrombosis.
Indications
Obtaining access for dialysis: involves the formation of a fistula two to three months prior to the start of dialysis. A native fistula should ideally be created as far away as feasible to minimize the risk of heart strain and "steal syndrome" while simultaneously providing the ideal length for venous cannulation and allowing for the eventual construction of more proximal access if necessary.
Signs of a leg fistula include: Occlusion of the innominate vein or superior vena cava (usually as a result of prior central vein lines).
Severe obesity, central venous blockage, or exhausted peripheral veins are indications for transplant fistulas.
Central vein catheters: Necessary in cases of severe heart failure, peripheral vascular disease, or emergency hemodialysate without a functional fistula.
Anatomy
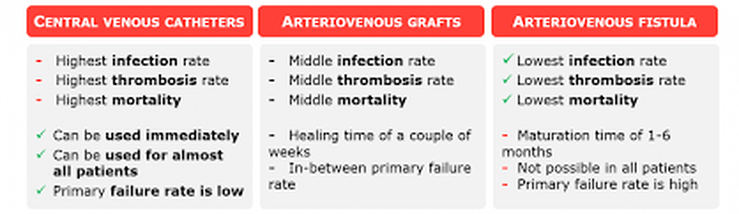
There are three primary methods available: central venous catheter, prosthetic arteriovenous graft, or native arteriovenous fistula (AVF).
Native fistulas: Brachiobasilic, brachiocephalic, atypical (ulnarbasilic or radiobasilic), more proximal radiocephalic (Brescia–Cimino), brachiocephalic, and upper leg (saphenous vein loop, saphenous vein in situ, and femoral vein loop).
Axillary artery to contralateral axillary vein (necklace graft), axillary loop graft, and contralateral IJV bypass graft are examples of complex vascular access operations. SFV transposition (SVC obstruction), femoro-femoral crossover bypass, and axillary artery-popliteal vein bypass graft (SVC obstruction in individuals with diabetes or obesity).
Catheters for the central vein: Single and dual lumen catheters, non-tunnelled (short-term) or tunnelled (cuffed to prevent infection).
Investigations
Thorough clinical evaluation of the venous and arterial anatomy prior to surgery. Allen examination. If necessary—for example, due to a history of vascular issues or assessment difficulties—duplex scanning can be used to evaluate vein patency, artery input, and caliber. Venogram in case the patency of the veins is in doubt.
Post-operative: Fistula assessment and clinical examination of bruit and thrill. Before native fistulae can be utilized for dialysis, they often need a few weeks to grow. One can needle grafts more rapidly.
Aftercare: measurement of the ultrasound dilution to gauge the cardiac output, recirculation rate, and graft input rate. A fistulogram and the required intervention, such as endovascular or surgical fistuloplasty of stenosis, can be carried out if the inflow is less than 600 ml/min, there has been a decline since the last evaluation, or the recirculation rate is greater than 5%.
Anaesthesia: Depending on the procedure, either a local, regional, or global block is used.
Procedure
The vein is evaluated, dissected, mobilized, and separated distally after the proper incision. After the artery is dissected and heparin is injected intravenously, it is clamped, and an arteriotomy is made. Prolene suture is used to perform a side-to-side anastomosis. For simple cannulation in brachiobasilic fistulae, the vein must be transferred into superficial subcutaneous tissue. The most common grafts utilized are looped, straight, or PTFE.
Catheters for the central vein: Internal jugular veins are typically utilized for placement under ultrasound guidance; femoral veins can be used, but only temporarily, because of the danger of thrombosis and infection.
Complications
Thrombosis, failure to mature, limb edema, aneurysmal dilatation, bleeding, infection, nerve injury, distal embolization, steal syndrome, and thrombosis.
0 Comments
